Introduction
Prostate cancer (PC) is the sixth leading of cancer-related mortality in men [1]: approximately one out of five men has a biochemical relapse after prostate cancer therapy [2]. Despite significant advances in the treatment of prostate cancer, the adaptive mechanisms of tumor cells in response to therapy remain largely unknown.
The role of autophagy has been noted in the development of malignant tumors at all stages of oncogenesis, from onset to tumor progression and outcome. Autophagy is the process of partial self-destruction of a damaged part of a cell to ensure its survival and recovery [3]. The existence of protective autophagy as one of the mechanisms of disease progression and resistance to treatment has been demonstrated [4, 5]. After induction by a stress signal, the autophagosome formation is the first step in autophagy process, in which LC3B protein (Microtubule-associated protein 1A/1B-light chain 3 phosphatidylethanolamine) plays a significant role by enhancing membrane fusion [6, 7]. There are scarce publications, in which an importance of autophagy markers for prostate cancer prognosis has been studied, but their role in relapse development remains poorly understood [8-10]. Some other published sources studied autophagy as a mechanism of adenocarcinoma cell survival after the antitumor therapy [11, 12].
Objective: To assess the immunohistochemical expression of the LC3B autophagy marker in tumor tissue before and after treatment with high-intensity focused ultrasound (HIFU) therapy and combined therapies: androgenic deprivation (AD)+ HIFU, AD + radiation therapy in patients with and without recurrent prostate adenocarcinoma.
Material and Methods
The study was carried out on biopsy material of prostates obtained from 70 patients with prostate adenocarcinoma before and after treatment.
The first group included 40 patients without signs of relapse after treatment, as evidenced by a normal blood PSA level, the results of ultrasound procedure and biopsy. In this group, 20 patients underwent treatment with High-intensity focused ultrasound ablation of the prostate (HIFU therapy), 20 patients underwent combined therapy: androgenic deprivation – AD + HIFU (10 patients), AD + radiation therapy (10 patients).
The second group included 30 patients with relapse of adenocarcinoma after treatment: 10 patients after HIFU therapy, 20 patients after combined therapy: AD + HIFU (10 patients) and AD + radiation therapy (10 patients). The relapse was confirmed by morphological examination of the biopsy material.
All biopsies after fixation and standard wiring were embedded in paraffin blocks. Tissue sections 4-5 μm thick made on a rotary microtome were stained with hematoxylin and eosin. Immunohistochemical studies were performed using Mouse and Rabbit Specific HRP/AEC IHC Detection Kit – Micropolymer System (Abcam, UK), diaminobenzidine as a chromogen. In all cases, the Anti-LC3B antibody ab48394 (dilution 1:200, Rabbit polyclonal to LC3B, Abcam) was used. The positive expression was assessed by dot staining of the cytoplasm and staining of cell nucleus. The reaction results were calculated using histochemical score (Hs).
Calculation formula: histochemical score (Hs) = ∑ P (i) x i, where “i” is the intensity of staining, expressed in points from 0 to 3 (0-no color, 1-weak, 2-moderate, 3-strong), P (i) is the percentage of stained cells.
The results are interpreted in terms of the following scale: Hs of 0-100 points correspond to weak reaction; 100-200 points indicate a moderate reaction; 200-300 points imply strong reaction. The maximum value of the histochemical count was 300.
Data processing was carried out using the SPSS 13.0 for Windows statistical data processing software package. Testing for normality of data distribution was performed by the Kolmogorov-Smirnov test. If the distribution of the studied parameters differed from normal, the methods of nonparametric statistics were used for comparative analysis. The Wilcoxon T-test was used to determine the significance of the differences between two dependent samples (before and after treatment). The significance of the difference was accepted at Р≤0.01.
Results
Before treatment, we observed the moderate cytoplasmic expression of LC3B marker in prostate adenocarcinoma cells (Hs=111) in the first group of patients (Table 1). The weak nuclear reaction in adenocarcinoma cells and a weak cytoplasmic expression in the cells of the muscle connective tissue stroma (Hs=47) were observed. In 10% of patients, there was a weak positive LC3B reaction in the vessel wall, mainly in endothelial cells (Hs=28).
Table 1. Expression of LC3B marker in patients with and without relapse of adenocarcinoma
|
Expression of LC3B (Hs) |
In the group without relapse |
In the group with relapse |
||
|
before treatment |
after treatment |
before treatment |
after treatment |
|
|
in adenocarcinoma cells |
111 (111, 115)* |
0* |
152 (138, 160)* |
260 (250, 285)* |
|
in the muscle connective tissue stroma |
47 (43, 50)* |
75 (68, 80)* |
44 (35, 52)* |
118 (100, 130)* |
|
in the vascular wall |
28 (20, 35)* |
55 (46, 60)* |
30 (25, 35) |
45 (30, 55) |
After HIFU ablation, the expression of anti-LC3B antibody was negative in adenocarcinoma cells, the weak cytoplasmic expression was observed in the stroma of muscle connective tissue (Hs=75) (Figure 1 А, B) and in the endothelium of vascular wall (Hs=59). In this group of patients, the intense extracellular expression in the muscle connective tissue stroma was noted 24 months after HIFU ablation (Figure 1D).
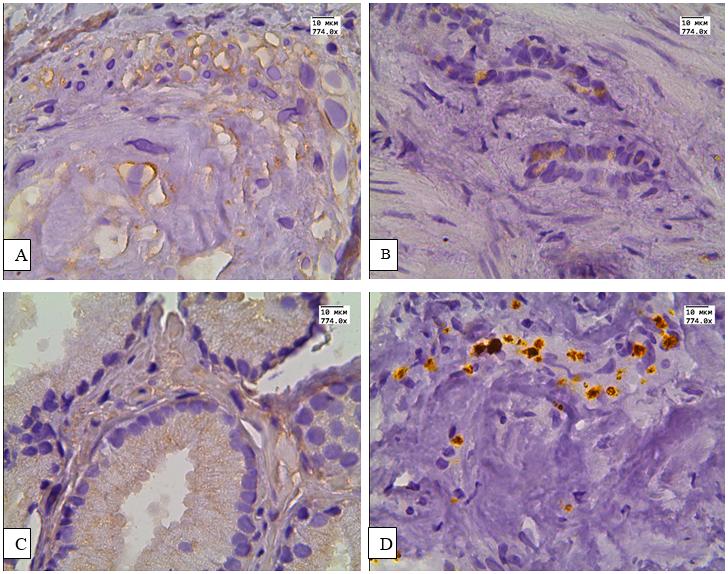
Figure 1. Expression of LC3B in the prostate tissue of adenocarcinoma patients without relapse after HIFU ablation and combined therapy. A – expression of LC3B in the muscle connective tissue stroma; B – expression of LC3B in the cytoplasm of epithelial cells and cells of the muscle connective tissue stroma; С – expression of LC3B in the cytoplasm of epithelial cells and cells of the muscle connective tissue stroma; D – expression of LC3B in the muscle connective tissue stroma after HIFU ablation. x774.
After combined therapy – AD + HIFU (Figure 1 C) and radiation therapy + AD, the expression of the LC3B marker in adenocarcinoma cells, muscle connective tissue and in the vascular wall was similar to that after HIFU ablation (Table 2). The differences in the expression of LC3B between groups with various types of treatment were insignificant according to the Wilcoxon T-test (Р>0.01).
Table 2. Expression of LC3B marker in patients with prostate adenocarcinoma after various treatments
|
Types of treatment |
In the group without relapse |
In the group with relapse |
||||
|
in adenocarcinoma cells |
in the muscle connective tissue stroma |
in the vascular wall |
in adenocarcinoma cells |
in the muscle connective tissue stroma |
in the vascular wall |
|
|
HIFU ablation |
0 |
80 (60, 85) |
59 (50, 70) |
280 (300, 300) |
140 (114, 155) |
30 (22, 38) |
|
AD + HIFU |
0 |
65 (50, 71) |
55 (45, 70) |
255 (200, 300) |
110 (87, 144) |
48 (29, 58) |
|
AD + radiation therapy |
0 |
70 (45, 100) |
45 (30, 50) |
265 (200, 300) |
130 (98, 148) |
43 (32, 50) |
The immunohistochemical expression of LC3B marker varied significantly in patients of the first group before and after treatment according to the Wilcoxon T-test. The significant differences in the expression were observed both in tumor cells (Temp<Tcr (0.01), z=5,46, P<0,001) and in cell cytoplasm of muscle connective tissue (Temp<Tcr (0.01), z=4,59, P<0,001) and vascular endothelium (Temp<Tcr (0.01), z=5,46, P<0,001).
In the second group of patients, LC3B expression was moderate in tumor tissue before treatment (Hs=145). The point cytoplasmic expression was observed in 89% of patients and it was localized mainly in the area closest to the cell membrane. In 7% of patients, a weak nuclear expression of this marker was observed in tumor cells. The expression was weak in the cells of the muscle connective tissue stroma (Hs=44), it was only noted in 12% of patients. In the endothelial cells, LC3B expression was weak (Hs=30) and it was observed in only 5% of patients.
After HIFU ablation, the cytoplasmic expression of LC3B marker was pronounced in tumor cells (Hs=280) in all patients of this group (Figure 2. А, B). The expression was moderate in muscle connective tissue stroma, and weak in the vascular wall (Hs = 140 and 30, respectively).

Figure 2. Expression of LC3B in the prostate tissue of adenocarcinoma patients with relapse after HIFU ablation. A – expression of LC3B in the cytoplasm of adenocarcinoma cells; B – еxpression of LC3B in the cytoplasm of adenocarcinoma cells and in the muscle connective tissue stroma of the prostate. х 774.
After combined therapy – AD + HIFU (Figure 3 A, B) and radiation therapy + AD (Figure 3 C, D), the expression of the LC3B marker in adenocarcinoma cells, muscle connective tissue and in the vascular wall was similar to that after HIFU ablation (Table 2). The differences in the expression of LC3B between groups with various types of treatment was insignificant according to the Wilcoxon T-test (Р>0.01).
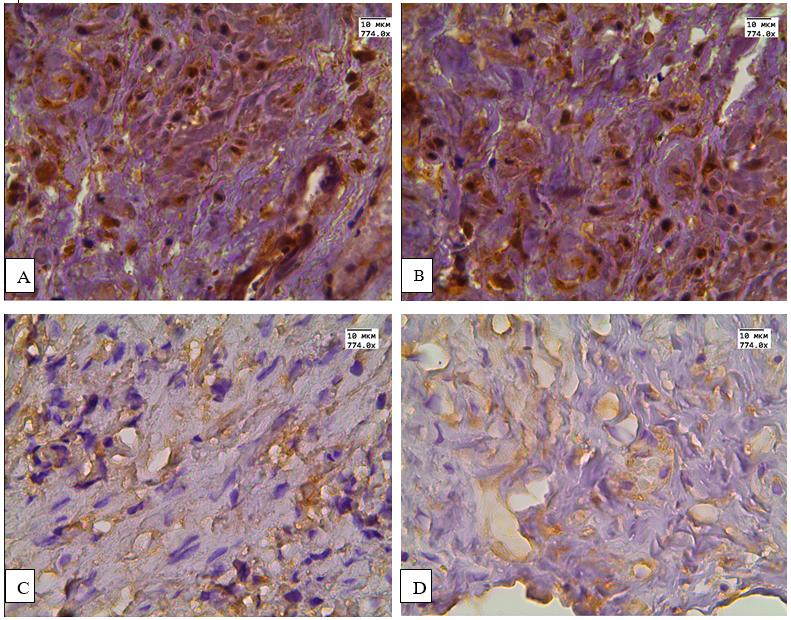
Figure 3. Expression of LC3B in the prostate of adenocarcinoma patients with relapse after combined therap. A, B – expression of LC3B in adenocarcinoma cells and muscle connective tissue stroma; C, D – expression of LC3B in the cells of the muscle connective tissue stroma and blood vessels. х774.
According to the Wilcoxon T-test, the expression of LC3B marker varied significantly in patients of the second group before and after treatment both in tumor cells (Temp<Tcr (0.01) z-4,71, P 0,000) and in the cells of the muscle connective tissue stroma (Temp<Tcr (0.01), z-4,59, P 0,000).
Discussion
In patients with prostate cancer, the cytoplasmic expression of the autophagy marker LC3B in tumor cells was moderate before treatment. The obtained data correspond to the results of other authors [13].
After treatment, the expression of the autophagy marker was negative in the tumor tissue in the group of patients without relapse, but it was pronounced in the cytoplasm of the cells of the muscle connective tissue stroma and in the endothelium, which indicates the processes of regeneration in the prostate stroma. In the group of patients with relapse of adenocarcinoma, we observed a significant increase in the expression of LC3B marker in tumor cells and in cells of the muscle connective tissue stroma after treatment. It should be noted that we observed nuclear expression of the marker only in those patients with relapse, who received combined therapy: AD + HIFU and AD + radiation therapy. This is probably due to the fact that androgen receptors located in the nucleus are one of the points of application in androgen deprivation [14, 15].
The expression of the autophagy marker was not dependent on the treatment method both in the first and the second groups of patients.
A significant increase of LC3B expression in tumor cells in the group of patients with relapse and the absence of this marker in patients without relapse is most likely due to the fact that autophagy is one of the mechanisms of tumor cell survival after the treatment. In current literature, some published sources emphasize the role of autophagy in the survival of tumor cells after treatment of cancer of other localizations [13]. Thus, an increase in the expression of autophagic proteins after treatment of patients with prostate adenocarcinoma may be an important prognostic marker of relapse.
Сonclusion
Regardless of the type of treatment, the expression of the autophagy marker LC3B decreased in adenocarcinoma cells in the group of patients without relapse and increased in the group of patients with relapse after treatment. In the connective tissue, stroma and the vessel wall, LC3B expression increased after treatment in both groups.
The autophagy is one of the factors contributing to the survival of prostate adenocarcinoma cells after treatment; the increase in autophagy marker LC3B expression after treatment in patients with prostate adenocarcinoma can be used to assess the risk of relapse.
Acknowledgments
The study was partially supported by the Public Procurement (No. 121032600197-2) of the Russian Federation Ministry of Healthcare.
Conflict of interest
none declared.
- EAU Guidelines. Edn. presented at the EAU Annual Congress Milan 2021. Arnhem, Netherlands: EAU Guidelines Office. http://uroweb.org/guidelines/compilations-of-all-guidelines.
- Glaser ZA, Rais-Bahrami S. Fluciclovine positron emission tomography in the setting of biochemical recurrence following local therapy of prostate cancer. Transl Androl Urol 2018; 7(5): 824-830. https://doi.org/10.21037/tau.2018.07.17.
- Niklaus M, Adams O, Berezowska S, Zlobec I, Graber F, Slotta-Huspenina J, et al. Expression analysis of LC3B and p62 indicates intact activated autophagy is associated with an unfavorable prognosis in colon cancer. Oncotarget 2017; 8(33): 54604-54615. https://doi.org/10.18632/oncotarget.17554.
- Eskelinen EL. Autophagy: supporting cellular and organismal homeostasis by self-eating. Int J Biochem Cell Biol 2019; 111: 1-10. https://doi.org/10.1016/j.biocel.2019.03.010.
- Yun CW, Lee SH. The Roles of Autophagy in Cancer. Int J Mol Sci 2018; 19(11): 3466. https://doi.org/10.3390/ijms19113466.
- Schläfli AM, Berezowska S, Adams O, Langer R, Tschan MP. Reliable LC3 and p62 autophagy marker detection in formalin fixed paraffin embedded human tissue by immunohistochemistry. Eur J Histochem 2015; 59(2): 2481. https://doi.org/10.4081/ejh.2015.2481.
- White E, Mehnert JM, Chan CS. Autophagy, Metabolism, and Cancer. Clin Cancer Res 2015; 21(22): 5037-5046. https://doi.org/10.1158/1078-0432.ccr-15-0490.
- Giatromanolaki A, Sivridis E, Mendrinos S, Koutsopoulos AV, Koukourakis MI. Autophagy proteins in prostate cancer: Relation with anaerobic metabolism and Gleason score. Urol Oncol 2014; 32(1): 39.e11-e18. https://doi.org/10.1016/j.urolonc.2013.04.003.
- Gabriele F, Martinelli C, Comincini S. Prostate cancer cells at a therapeutic gunpoint of the autophagy process. J Cancer Metastasis Treat 2018; 4: 17. https://doi.org/10.20517/2394-4722.2018.06.
- Cristofani R, Montagnani Marelli M, Cicardi ME, Fontana F, Marzagalli M, Limonta P, et al. Dual role of autophagy on docetaxel-sensitivity in prostate cancer cells. Cell Death Dis 2018; 9(9): 889. https://doi.org/10.1038/s41419-018-0866-5.
- Li YJ, Lei YH, Yao N, Wang CR, Hu N, Ye WC, et al. Autophagy and multidrug resistance in cancer. Chin J Cancer 2017; 36(1): 52. https://doi.org/10.1186/s40880-017-0219-2.
- Mortezavi A, Salemi S, Kranzbühler B, Gross O, Sulser T, Simon HU, et al. Inhibition of autophagy significantly increases the antitumor effect of Abiraterone in prostate cancer. World J Urol 2019; 37(2): 351-358. https://doi.org/10.1007/s00345-018-2385-5.
- Hashimoto D, Bläuer M, Hirota M, Ikonen NH, Sand J, Laukkarinen J. Autophagy is needed for the growth of pancreatic adenocarcinoma and has a cytoprotective effect against anticancer drugs. Eur J Cancer 2014; 50(7): 1382-1390. https://doi.org/10.1016/j.ejca.2014.01.011.
- Mortezavi A, Salemi S, Rupp NJ, Rüschoff JH, Hermanns T, Poyet C, et al. Negative LC3b immunoreactivity in cancer cells is an independent prognostic predictor of prostate cancer specific death. Oncotarget 2017; 8(19): 31765-31774. https://doi.org/10.18632/oncotarget.15986.
- Maslyakova GN, Voronina ES, Bucharskaya AB, Medvedeva AV. Therapeutic patomorphosis of prostate adenocarcinoma in 3 months after the maximal androgenic blockade. Modern problems of science and education 2017; (4): 29. Russian. https://elibrary.ru/item.asp?id=32663050.
Received 10 November 2020, Revised 15 September 2021, Accepted 21 December 2021
© 2020, Russian Open Medical Journal
Correspondence to Alla B. Bucharskaya. Address: 112 Bolshaya Kazachya St., Saratov 410012, Russia. Phone: +79053850895. E-mail: allaalla_72@mail.ru.