Introduction
Coronary revascularization with coronary artery bypass grafting (CABG) is preferable compared with pharmacological treatment for controlling the symptoms of myocardial ischemia and preventing the myocardial infarction (MI) [1]. Perioperative CABG-associated complications are known predictors of higher mortality in patients with stable coronary artery disease (SCAD) [2]. Postoperative cognitive dysfunction (POCD), implying patient’s memory and learning decline after surgery, is among significant complications, and is found in 10-50% post-CABG patients, depending on used diagnostic criteria [3, 4].
Prognostic tools and minimization of the POCD risk imply screening of risk factors for cerebral ischemia, such as asymptomatic carotid stenosis [5], and modification of surgical approach [6], if suitable. There are contradictory data on the impact of different perfusion strategies, i.e. on-pump CABG versus off-pump CABG, on POCD. Limited evidence exists that there is no difference in incidence and severity of cognitive decline between on-pump and off-pump CABG [7], and that it is comparable with pharmacological treatment [8]. POCD is a proven predictor of long-term risk of dementia and shorter longevity in post-CABG patients [9, 10]. All analyses demonstrate results obtained on low surgical risk cohorts. Therefore, severity, duration of POCD, its reversibility and risk factors in off- and on-pump patients with SCAD and planned low surgical risk CABG are currently insufficiently studied.
The objective of the current study was to analyze incidence, severity, and risk factors for postoperative cognitive decline in low-risk patients undergoing elective CABG.
Material and Methods
Personal medical records of 79 repeated patients (mean age of 61.1±6.0 years) were retrospectively analyzed. All patients underwent elective CABG without hypothermia, either on-pump (44 patients) or off-pump (35 patients).
Inclusion criteria: elective CABG for SCAD treatment, secondary education.
Exclusion criteria: personal history of brain injury, diagnosed mental disorders, substance abuse, psychopharmacotherapy prescribed before CABG.
Duration of post-CABG observation was 6 months. Mini-mental state examination (MMSE), Montreal cognitive assessment (MoCA) test, Stroop test and trail making test (TMT) were used to assess cognitive status (for all tests, the authors used validated versions in Russian language). Aerobic exercise tolerance was assessed using six-minute walk test. Scores were interpreted according to the original instructions. The social and demographic characteristics of the cohort are presented in Table 1.
Table 1. Baseline social and demographic characteristics.
|
Parameter |
Incidence, % |
|
Females |
70 |
|
Marital status |
|
|
Married |
71 |
|
Divorced |
23 |
|
Widow |
6 |
|
Disability due to somatic conditions |
|
|
None |
96 |
|
grade 3 |
1 |
|
grade 2 |
2 |
|
Children |
|
|
No |
7 |
|
1 child |
91 |
|
2 children or more |
2 |
|
Education |
|
|
School |
1 |
|
College |
6 |
|
Incomplete higher education |
48 |
|
Complete higher education |
45 |
Data were collected before operation, 8 days, 3 weeks, 3 months, and 6 months post-CABG. None of the participants died or were excluded from the study during the observation period.
Statistical analyses
Statistical processing was performed using SPSS 23.0 (IBM Inc., USA). Kolmogorov-Smirnov criterion was used to test for normality of the distribution. Parametric two-way ANOVA or nonparametric Mann-Whitney U test were used to compare the groups. Using Kolmogorov-Smirnov test meant for n≥50, the data were determined to be nonparametric; hence, Spearman’s correlation coefficient was used.
Results
Baseline characteristics of non-modifiable risk factors
The baseline medical characteristics of the general cohort are shown in Table 2. There was no difference between on-pump and off-pump CABG patients in the number of patients with a history of stroke (7% and 14%, respectively, p=0.35), PCI (12% and 15%, p=0.67) or AF (13% and 8%, p=0.43). Mean number of grafts per patient was 2.4±0.9 for the on-pump and 2.6±0.7 for the off-pump group (p=0.43). EuroSCORE II risk was higher in patients with longer duration of aortic clamping (r=0.28, p=0.048). Mean EuroSCORE II risk was 1.10±0.64% in off-pump group and 1.07±0.77% in on-pump group (p=0.86); all patients in both groups were considered low surgical risk. Mean pre-CABG result of a six-minutewalk test in off-pump and on-pump groups was 352±39 m and 356±36 m, respectively (p=0.70).
Table 2. Characteristics of somatic conditions in participants
|
Condition |
Prevalence/severity |
|
Arterial hypertension, %. Including: |
98 |
|
Grade 2 hypertension, % |
21 |
|
Grade 3 hypertension, % |
63 |
|
Personal history of MI, % |
67 |
|
Mean CCS angina class, M±m |
2.53±0.91 |
|
History of percutaneous coronary interventions (PCI), % |
14 |
|
Dyslipidemia, % |
63 |
|
History of stroke, % |
14 |
|
Type 2 diabetes, %. Including |
39 |
|
Insulin treatment, % |
9 |
|
Lower limb artery disease, % |
5 |
|
Mean BMI, kg/m2, M±m |
29.3±4.2 |
|
Mean NYHA heart failure class, M±m |
1.73±0.73 |
|
History of atrial fibrillation (AF), % |
17 |
|
Paroxysmal AF, % |
10 |
|
Chronic obstructive pulmonary disorder, % |
6 |
|
Peripheral oxygen saturation at rest <95%, % |
3 |
|
Renal failure, % |
9 |
|
Mean number of grafts per patient, M±m |
2.5±0.8 |
|
Mean EuroSCORE II risk, M±m |
1.08±0.71 |
Pre- and postoperative markers of cognitive functioning
Table 3 represents data on severity of pre- and posteoperative cognitive dysfunction assessed with MMSE and MoCA.
Table 3. Cognitive impairment of patients before and after CABG
|
Marker |
Incidence, % |
|
|
Pre-CABG |
6 months after CABG |
|
|
MMSE: |
||
|
Normal (29-30 points) |
20 |
17 |
|
Mild cognitive decline (28 points) |
19 |
22 |
|
Moderate cognitive decline (25-27 points) |
41 |
44 |
|
Mild dementia (20-24 points) |
20 |
17 |
|
MoCA: |
||
|
Normal (26 points and more) |
50 |
52 |
|
Cognitive decline (25 points or less) |
50 |
48 |
Markers of cognitive impairment were found in half of the patients. In the vast majority of cases, it was classified as moderate cognitive impairment. At the same time, rates of cognitive dysfunction were comparable pre-CABG and 6 months post-CABG (Table 3). Mean MMSE score corresponds to moderate cognitive decline in both on-pump and off-pump groups. Mean pre-operation MоCA score was ‘normal’ in the on-pump group and ‘cognitively reduced’ in the off-pump group (Table 4).
Table 4. Baseline markers of cognitive functioning in off-pump and on-pump patients
|
Score |
On-pump |
Off-pump |
General cohort |
Inter-group P-value |
|
Mean pre-CABG MMSE score, M± m |
26.4±2.6 |
25.9±2.6 |
26.2±2.6 |
0.44 |
|
Mean pre-CABG MoCA score, M± m |
26.0±2.5 |
24.5 ±3.1 |
25.3±2.8 |
0.097 |
There was a positive correlation between MMSE and MoCA scores (r=0.79, p<0.001 pre-CABG, r=0.85, p<0.001 at 8 days post-CABG, r=0.80, p<0.001 at 3 weeks, r=0.93, p<0.001 at 3 months, r=0.96, p<0.001 at 6 months).
POCD in off-pump patients was more pronounced, compared with the on-pump patients, yet there was no difference in the measurements at the end of the observation period (Table 5).
Table 5. Aerobic physical tolerance and cognitive functioning in off-pump and on-pump patients
|
Parameter |
Average for all patients |
On-pump |
Off-pump |
Statistical significance of differences between off-pump and on-pump patients |
|
6 min walk test increase at 6 months, m, M±m |
+114.1±83.9 |
+120.0±100.6 |
+101.7±27.4 |
0.55 |
|
MMSE change at 8 days post-CABG, points, M±m |
-1.5±2.7 |
-0.9±3.2 |
-2.4±1.6 |
0.104 |
|
MMSE decreased by >2 points at 8 days, % |
43 |
35 |
53 |
0.13 |
|
MMSE change at 3 weeks post-CABG, points, M±m |
-0.1±2.2 |
0.5±2.5 |
-1.0±1.4 |
0.045 |
|
MMSE change at 6 months post-CABG, points, M±m |
-0.4±1.2 |
-0.2±1.2 |
-0.7±1.5 |
0.67 |
|
MoCA change at 8 days post-CABG, points, M±m |
-2.9±2.1 |
-2.2±2.0 |
-3.9 ±2.0 |
0.018 |
|
MoCA decreased by >3 points at 8 days, % |
44 |
32 |
60 |
0.032 |
|
MoCA change at 3 weeks post-CABG, points, M±m |
-0.6±1.4 |
-0.2±1.4 |
-1.3 ±1.1 |
0.018 |
|
MoCA change at 6 months post-CABG, points, M±m |
-0.6±1.7 |
0±1.1 |
-1.8 ±2.4 |
0.099 |
The duration of POCD course after CABG was 3 weeks measured by the time with significant differences between baseline and postoperative cognitive measurements. Differences between baseline results and those on day 8 after the CABG were significant at p<0.001 for both MMSE and MoCA tests, reaching p=0.16 for MMSE and p=0.015 for MoCA at 3 weeks point.
Baseline MoCA score <25 was a good predictor for more pronounced cognitive decline measured by MoCa at 8 days point (decline was 3.9±1.4 in lower MoCA group and 2.5±2.3 in higher MoCA group, p=0.038), but no such correlation was observed at 3 weeks (change in MoCA was 0.35±1.15 and 1.3±1.7, respectively, p=0.16). No association between baseline and postoperative MMSE levels was found.
In on-pump group, duration of the perfusion was not associated with severity or prevalence of POCD. Also, no association was found between POCD and age, grade of hypertension, personal history of diabetes, MI or stroke.
Each subsequent exercise test demonstrated longer distance compared with the previous one (p<0.001 for every test-to-test comparison), with comparable increases in off-pump and on-pump groups (Figure 1).
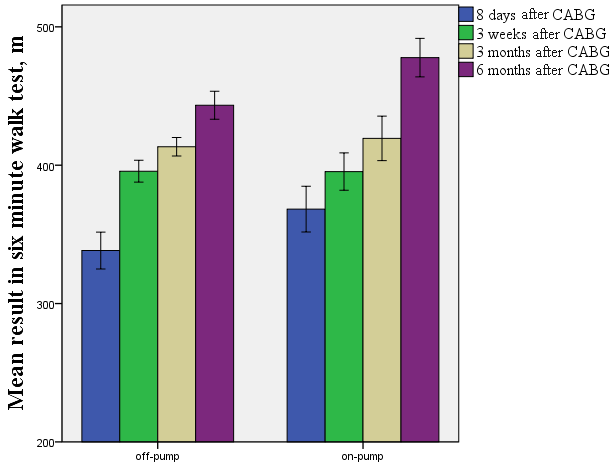
Figure 1. Change in the exercise tolerance in off-pump and on-pump patients.
POCD severity was not associated with changes in 6 min walk test results during the observation period.
Executive functions after CABG
Patients were evaluated with TMT and Stroop test at day 8 post-CABG to assess their executive functions.
Our results demonstrated that 29% patients needed less than 79 sec to pass TMT, part A (temporal criterion for intact cognitive functions); 97% patients passed TMT, part B, in less than 279 sec. In Stroop test, mean difference between time needed to complete table 2 and table 3 was 72.7±36.3 sec, and difference between part 2 and part 1 was 1.4±0.3 sec. Results of both tests were similar for on-pump and off-pump groups. They also did not correlate with the duration of operation, severity of MMSE and MoCA decrease at day 8, or with baseline MMSE and MoCA volumes.
Discussion
In this paper, we present the results of retrospective assessment of cognitive functions after elective low-risk CABG in patients with SCAD. In contrast to the evidence from higher-risk cohorts [11], in this study, performed in low-risk patients, EuroSCORE II was shown ineffiective as POCD predictor. Details of personal history, i.e., stroke, MI and diabetes, did not demonstrate association with the course of POCD as well. Therefore, in POCD risk stratification for low-risk cohort, the priority should be given to the cognitive function assessment.
Even in low-risk elective CABG group, over 40% patients demonstrate substantial transient decrease in MMSE and MoCA tests, which is close to the estimates from other population-based registries [4, 11]. Our data matched the results of the meta-analysis [12] in the duration of POCD and its reversibility in mid-term. While MMSE is mostly used for verification of dementia, MoCA test was performed and validated for screening of cognitive impairment of mostly moderate severity [13, 14]. According to the validation studies, MoCA sensitivity and specificity in diagnosing mild cognitive impairment was 90% and 87%, respectively. MMSE demonstrated rates of 18% and 100%, respectively [15]. Both scales demonstrated comparable diagnostic accuracy in the screening of dementia [14, 16]. According to our data, in most cases POCD was limited to mild cognitive impairment, and MoCA was a more sensitive prognostic tool of POCD. Therefore, pre-CABG evaluation with MoCA and subsequent control re-tests seems a more effective way of POCD screening in patients undergoing elective low-risk CABG. According to our data, the optimal threshold of pre-CABG MoCA score is 25 points with lower results indicating higher risk of POCD. Our data demonstrated superiority of on-pump CABG over off-pump operation in respect with the risks of POCD in low-risk population.
Limitations of this study include small sample size and absence of pre-CABG data on executive cognitive functioning. Currently, there is no data on long-term outcomes. Because this was single-center study, the data on preferable on-pump CABG require validation on larger multi-center registries and should not be extrapolated on higher-risk CABG cohorts. Further prospective trials are needed to evaluate the efficacy of the guided screening POCD prevention.
Conclusion
POCD risk differs in off-pump and on-pump CABG cohorts, with significantly higher prevalence in the former group – no matter, whether assessed with MMSE or MoCA tests. Differences are observed within 3 weeks post-CABG. No evidence was found that POCD symptoms persist within months after surgery in the majority of these patients.
Pre-CABG MoCA score <25 is associated with more pronounced POCD in low-risk elective CABG cohort, and these patients should be monitored for neurological complications more scrupulously.
Acknowledgements
The authors would like to thank all patients recruited in the study for their participation. We are also grateful for Dr. Mariia Dorofeikova’s valuable critical comments in the course of the preparation of this manuscript.
Conflict of Interest
The authors declare no conflicts of interest.
Ethical approval
Design of this clinical trial was retrospective. Formal consent was not required for this type of study.
- Rezende PC, Hueb W, Garzillo CL, Lima EG, Hueb AC, Ramires JA, et al. Ten-year outcomes of patients randomized to surgery, angioplasty, or medical treatment for stable multivessel coronary disease: effect of age in the Medicine, Angioplasty, or Surgery Study II trial. J Thorac Cardiovasc Surg 2013; 146(5): 1105-1112. https://doi.org/10.1016/j.jtcvs.2012.08.015.
- Van Dijk D, Spoor M, Hijman R, Nathoe HM, Borst C, Jansen EW, et al. Cognitive and cardiac outcomes 5 years after off-pump vs on-pump coronary artery bypass graft surgery. JAMA 2007; 297(7): 701-708. https://doi.org/10.1001/jama.297.7.701.
- Mehta A, Gleason T, Wechsler L, Winger D, Wang L, Thirumala PD. Perioperative stroke as a predictor of mortality and morbidity in patients undergoing CABG. J Clin Neurosci 2017; 44: 175-179. https://doi.org/10.1016/j.jocn.2017.06.035.
- Kennedy ED, Choy KC, Alston RP, Chen S, Farhan-Alanie MM, Anderson J, et al. Cognitive outcome after on- and off-pump coronary artery bypass grafting surgery: a systematic review and meta-analysis. J Cardiothorac Vasc Anesth 2013; 27(2): 253-265. https://doi.org/10.1053/j.jvca.2012.11.008.
- Masabni K, Raza S, Blackstone EH, Gornik HL, Sabik JF 3rd. Does preoperative carotid stenosis screening reduce perioperative stroke in patients undergoing coronary artery bypass grafting? J Thorac Cardiovasc Surg 2015; 149(5): 1253-1260. https://doi.org/10.1016/j.jtcvs.2015.02.003.
- Raja SG, Garg S, Rochon M, Daley S, De Robertis F, Bahrami T. Short-term clinical outcomes and long-term survival of minimally invasive direct coronary artery bypass grafting. Ann Cardiothorac Surg 2018; 7(5): 621-627. https://doi.org/10.21037/acs.2018.06.14.
- Greaves D, Psaltis PJ, Davis DHJ, Ross TJ, Ghezzi ES, Lampit A, et al. Risk factors for delirium and cognitive decline following coronary artery bypass grafting surgery: a systematic review and meta-analysis. J Am Heart Assoc 2020; 9(22): e017275. https://doi.org/10.1161/JAHA.120.017275.
- Guan Z, Guan X, Gu K, Lin X, Lin J, Zhou W, et al. Short-term outcomes of on- vs off-pump coronary artery bypass grafting in patients with left ventricular dysfunction: a systematic review and meta-analysis. J Cardiothorac Surg 2020; 15(1): 84. https://doi.org/10.1186/s13019-020-01115-0.
- Klinger RY, James OG, Wong TZ, Newman MF, Doraiswamy PM, Mathew JP. Cortical β-amyloid levels and neurocognitive performance after cardiac surgery. BMJ Open 2013; 3(9): e003669. https://doi.org/10.1136/bmjopen-2013-003669.
- Evered LA, Silbert BS, Scott DA, Maruff P, Ames D. Prevalence of dementia 7.5 years after coronary artery bypass graft surgery. Anesthesiology 2016; 125(1): 62-71. https://doi.org/10.1097/ALN.0000000000001143.
- Tsai MF, Tsay SL, Moser D, Huang TY, Tsai FC. Examining symptom trajectories that predict worse outcomes in post-CABG patients. Eur J Cardiovasc Nurs 2019; 18(3): 204-214. https://doi.org/10.1177/1474515118809906.
- Greaves D, Psaltis PJ, Ross TJ, Davis D, Smith AE, Boord MS, et al. Cognitive outcomes following coronary artery bypass grafting: A systematic review and meta-analysis of 91,829 patients. Int J Cardiol 2019; 289: 43-49. https://doi.org/10.1016/j.ijcard.2019.04.065.
- Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005; 53(4): 695-699. https://doi.org/10.1111/j.1532-5415.2005.53221.x.
- Thomann AE, Goettel N, Monsch RJ, Berres M, Janh T, Steiner LA, et al. The Montreal Cognitive Assessment: normative data from a german-speaking cohort and comparison with international normative samples. J Alzheimers Dis 2018; 64(2): 643-655. https://doi.org/10.3233/JAD-180080.
- Pinto TCC, Machado L, Bulgacov TM, Rodrigues-Júnior AL, Costa MLG, Ximenes RCC, et al. Is the Montreal cognitive assessment (MoCA) screening superior to the mini-mental state examination (MMSE) in the detection of mild cognitive impairment (MCI) and Alzheimer's Disease (AD) in the elderly? Int Psychogeriatr 2019; 31(4): 491-504. https://doi.org/10.1017/S1041610218001370.
- Lee YC, Lin YT, Chiu EC. A comparison of test-retest reliability of four cognitive screening tools in people with dementia. Disabil Rehabil 2021; 9: 1-6. https://doi.org/10.1080/09638288.2021.1891466.
Received 22 May 2021, Revised 14 November 2021, Accepted 1 February 2022
© 2021, Russian Open Medical Journal
Correspondence to Sergei F. Zadvorev. Address: City Multifield Hospital No.2, 5 Uchebnyi Pereulok, Saint Petersburg 194354, Russia. Phone: +79533410803, E-mail: zadvoryevsf@yandex.ru.