Introduction
Orofacial clefts are among the most frequent congenital anomalies with a higher prevalence at birth than neural tube defects, but lower than cardiovascular malformations [1, 2, 3]. In Europe, the combined prevalence of cleft palate (CLP) and cleft lip (CL) at birth is approximately 1 in 700 live births, with certain ethnic and geographic variations [4]. It is believed that the pathogenesis of CL and/or CLP involves both genetic and environmental factors [5, 6]. Moreover, the disorders of maxillofacial region occupy a special place within a large group of congenital abnormalities due to severity of their clinical manifestations, as well as substantial socio-psychological impact on children [7, 8].
The outcomes of surgical interventions for congenital disorders of maxillofacial region greatly depend on the ability of postoperative tissue regeneration. To restore normal functions of the upper lip, it is not sufficient to just recreate its anatomical integrity; it is also necessary to restore the balance of muscle functioning in the region in order to ensure freedom and fullness of upper lip movements. However, postoperative scarring of the upper lip often suddenly reduces its functionality, thereby causing the dysfunction of the orbicularis oris muscle. Later in life, this disorder may interfere with normal articulation. Lip deformity may lead to the social and psychological maladjustment of a child. Despite continuously improving cheiloplasty/cheilorhinoplasty techniques, along with pharmacological and other wound healing technologies, an incidence of long-term postoperative complications of this pathology remains quite high [9, 10]. As a result, an absolute majority of primary patients who underwent cheilorhinoplasty require repeated corrective interventions [11, 12].
The inefficiencies of surgical corrections of CL and/or CLP complications, as well their prevention, are largely due to insufficient knowledge of the mechanisms of their development. The causes of postoperative complications are likely to be different in different periods of a healing process, and may depend on the extent of surgical trauma and child’s age. Genetically predetermined features of tissue reaction to surgical trauma [13], infectious process in the wound, as well as activation of potential pathogens due to postoperative immunodeficiency, may also be involved [14, 15]. Besides, anomalous hyper- and hypoinflammatory reactions may affect wound healing process [16].
Even though research of various prospects for improving an outcome of regeneration processes was actively explored over the past decades (including consideration of individual polymorphism of genes potentially involved in a healing process [17]), our study did not provide results directly relevant to clinical practices.
It is also known that tissues, injured after any surgical intervention, cause the release of cytokines, prostaglandins and other mediators in charge of activating nonspecific immune response with an involvement of leukocytes, platelets, endothelial cells, and extracellular matrix [18]. Such kind of response inevitably results in oxidative processes, physiologically aimed at cleansing necrotic tissues while stimulating granulation and epithelialization. Such reaction includes activation of leukocytes and may lead to excessive release of free radicals causing an oxidative tissue damage [19, 20]. On the other hand, a sharp drop in radical formation was presumed to contribute to the development of infectious processes on wound surfaces [16, 21].
It has also been demonstrated that changes in the mediator system, which regulates the course of inflammatory and regenerative reactions, are primarily associated with the extensive production of proinflammatory cytokines, such as interleukin-1β (IL-1β) and Tumor Necrosis Factor-α (TNFα), causing the disbalance of a normal ratio between proinflammatory and anti-inflammatory mediators, as well as altered concentrations of fibrogenic growth factors, such as Transforming Growth Factor-β (TGF-β) [18, 22]. An augmented physical pressure during the postoperative wound closure may lead to the damage of intracellular cytoskeleton of fibroblasts, thereby causing an overexpression of TGF-β and other cytokine genes, overdeveloped matrix formation, and hypertrophic scar development [23, 24].
The present-day concept of scar formation also considers an involvement of mast cell activation, which are present in large numbers in hypertrophic scars. These cells contribute to the scarring process by initiating excessive collagen formation due to secretion of histamine, which promotes vasodilation and the exit of plasma proteins into the extracellular space [25].
Anatomical anomalies of nasopharyngeal area in patients with congenital disorders of maxillofacial region result in imbalanced microbiota there [26]. This leads, in particular, to developing inflammatory diseases of oronasopharyngeal area [27]. The chronic inflammation, in turn, affects the condition of mucosal surfaces [28]. The continuous persistence of potential pathogens, such as Staphylococcus aureus, at mucosal surfaces promotes formation of pathogenic biofilm, which affects local immunity processes and may, therefore, be considered a leading pathogenic factor of inflammatory complications [29].
In regard to that, currently available data indicate that one of the main causes of hyperergic postoperative tissue response is a prolonged opening in the septum between normally separated anatomical regions, e.g., the nasal cavity and oropharynx. This would lead to the development of anomalous microbiota, i.e., non-characteristic for both sites.
Hence, the objective of our study was to determine possible interrelations between the composition of culturable facultative anaerobic microbiota of oronasopharyngeal mucosae and cytokine profiles in patients with congenital disorders of maxillofacial region in both pre- and postoperative periods.
Material and Methods
Study subjects
Our study was based on the results of examining 15 children (8 girls, 7 boys, 9-12 months of age) with unilateral congenital CL before surgical operation and 17 children (11 girls, 6 boys, 1-3 years of age) with unilateral congenital CL; 16 children (7 girls, 9 boys, 8-12 months of age) with unilateral congenital CLP before surgical operation and 22 children 1.5-3 years old who underwent primary cheilorhinoplasty. The surgery involved either the reconstruction of upper lip (CL patients), or the reconstruction of upper lip and elimination of unilateral flattening of the nose ala on the side of the cleft (CLP patients). The control groups for examining normal blood levels of cytokines consisted of healthy donors of matching ages, 15 children in each.
Signed informed consent was obtained from the parents. The study design was approved by the Ethics Committee at Kabardino-Balkarian State University. Patient data entry for subsequent analysis was carried out in anonymous mode, with each patient assigned an individual number. The study was conducted in compliance with the Russian Federation Law of December 30, 2017, based on Declaration of Helsinki and its later amendments.
Immunological and biophysical methods
To isolate leukocytes, blood (2-5 mL) was taken on an empty stomach from ulnar vein into siliconized polypropylene tubes with EDTA as anticoagulant. Blood was layered upon an equal volume of ficoll-verografin (with a specific gravity of 1.199 g/cm3) and centrifuged at 400 g for 40 minutes to collect leukocytes in interphase. The cells were transferred into the tube, washed twice by centrifugation (400 g, 10 minutes), counted, and the concentration of cells was adjusted to 106 cells/mL.
To obtain blood plasma, peripheral venous blood was collected on an empty stomach from the cubital vein into sterile siliconized polypropylene tubes with EDTA as anticoagulant. Stabilized blood was centrifuged at 400g for 5 minutes, and resulting supernatant was collected.
To study cytokines of the mucosae of mouth, nose and pharynx, sterile dental pins were used as previously described [30]. The pins were applied to the surfaces for 30 s then placed into Eppendorf tubes with 1 mL of sterile saline for 40 min. After that, pins were removed and solutions were evaluated for cytokine activity.
Antioxidant activity of blood plasma was determined sensu Vasiljeva et al. [31].
To investigate the content of IL-1β and interleukin 10 (IL-10) in blood serum and mucosal samples, ELISA kits were used (Vector Best, Russia). The test sample, 30 μL, was added to same amount of incubation buffer and kept at room temperature for 45 minutes. Then, the content of wells was removed, and the wells were rinsed four times. Biotinylated conjugate (100 μL) was added, and the mixture was kept at room temperature for two hours. Following the incubation, the sample was rinsed four times, followed by the additions of a chromogenic solution; and after a 30-minute incubation, 100 μL of stop solution was added, and the optical density was read at 450 nm.
Microbiological methods
The study of culturable microbiota was conducted on patients before the surgery and then at one, three, six, and twelve months after it. The isolation of pure bacterial cultures was performed by conventional bacteriological methods, followed by identification via MALDI-TOF Biotyper (Bruker, Germany).
Statistical analysis
The normality of data was tested using the online tool, AI-Therapy Statistics, at https://www.ai-therapy.com/psychology-statistics/distributions/normal, which generated histograms, a Q-Q plots, calculated skewness, kurtosis and performed Kolmogorov-Smirnov and Shapiro–Wilk tests for normality. Then, Student’s t-test was employed in MS Excel. P-value of less or equal 0.05 implied statistical significance. The microbial counts were converted to log10 of the number of viable bacterial colony forming units (CFU) per mL. The results were presented as means ± their standard deviations.
Results
Microbiological features of oronasopharyngeal mucosa in patients with congenital disorders of maxillofacial region
We discovered that the level of total microbial colonization of oronasopharyngeal mucosa of CL patients in preoperative period was 3.5±0.5 log СFU/mL, but it was not significantly different from microbial counts in healthy children (p=2.074). However, in children with CLP, total microbial counts of mucosae of the mouth, pharynx, and nose were significantly higher (4.5±0.5 log CFU/mL) than in healthy children of age-matching group (2.5±0.5 log CFU/mL, p<0.05) (Figure 1).
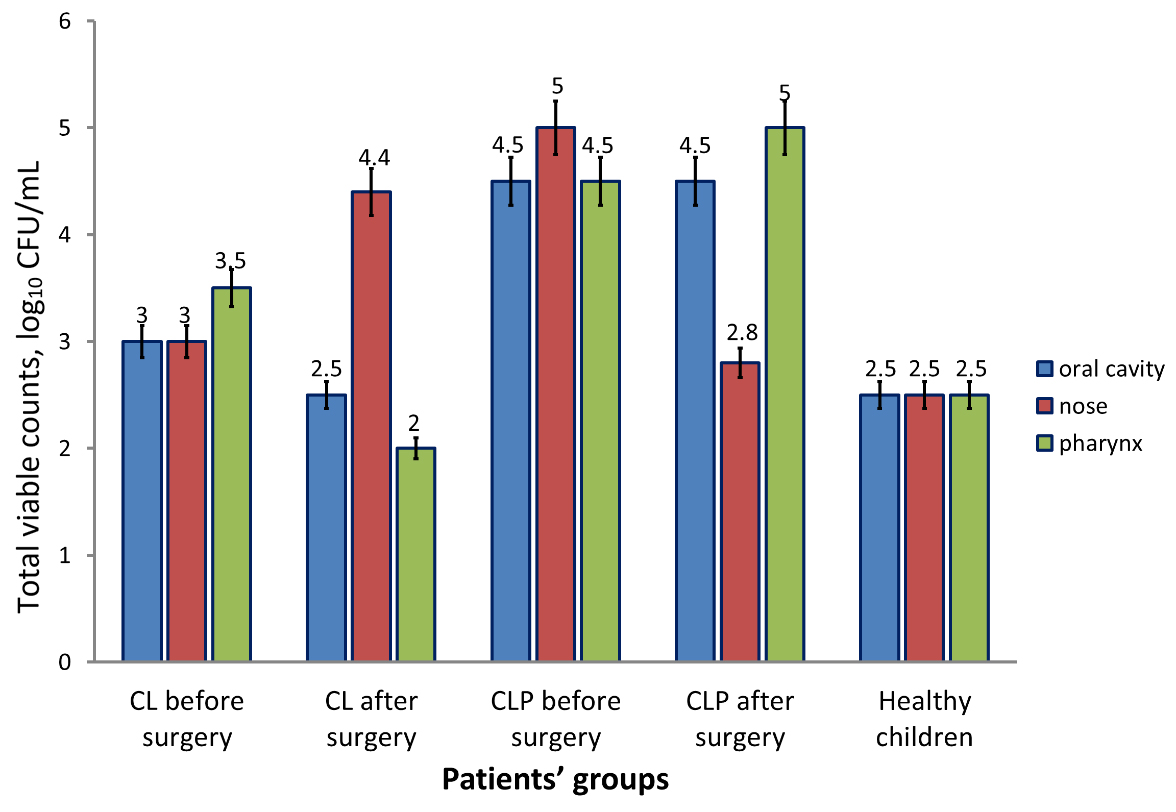
Figure 1. Total viable counts of culturable microbiota of oral, nasal and pharyngeal mucosae in children with CL and CLP in preoperative and postoperative periods. The numbers indicate means of log CFU/mL within each group and location. Error bars represent confidence intervals. CL, children with unilateral congenital cleft of upper lip; CLP, children with unilateral congenital cleft of upper lip and palate; CFU, colony forming unit.
To assess the presence and severity of dysbiotic changes, we determined the frequency of potentially pathogenic and pathogenic microorganisms in nasal, pharyngeal and oral microbiotas. Among the strains of potentially pathogenic species, Klebsiella pneumoniae and Candida albicans were the most frequent isolates, while top pathogenic representative of mucosal microbiotas in nasal, pharyngeal and oral cavities was S. aureus. In some cases, α-hemolytic streptococci were isolated (Streptococcus pneumoniae). None of these microorganisms were isolated from healthy children (Table 1). The possible explanation for this finding was the presence of abnormal opening between oral and nasal cavities, creating specific microenvironmental conditions at both biotopes, thereby causing the development of deteriorated microbiota (i.e., dysbiosis). On the other hand, we established an increased frequency (5%) of yeast-like fungi in healthy children without clinical signs of dysbiosis, compared with 0% in children of comparable age with CL; even though, before the surgery, children with CLP exhibited elevated levels of Candida spp. These findings imply an urgent need for further research to determine the cause of increased Candida spp. frequency.
Table 1. Potentially pathogenic microorganisms in oronasopharyngeal region of children with congenital disorders of maxillofacial region before and after surgery
|
Patient groups |
Isolation frequency, % |
|||
|
S. aureus |
K. pneumoniae |
S. pneumoniae |
C. albicans |
|
|
Children with CL before surgery |
36.4 |
9.1 |
0 |
0 |
|
Children with CL after surgery |
33.3 |
0 |
0 |
0 |
|
Children with CLP before surgery |
63.3 |
12.2 |
12.2 |
16.3 |
|
Children with CLP after surgery |
16.3 |
0 |
0 |
0 |
|
Healthy children (control) |
0 |
0 |
0 |
5.0 |
In postoperative period, total viable counts of microorganisms normalized, except for the microbiota of nasal cavity, but only in CL patients, whereas in the group of operated CLP children, the counts remained significantly higher (p<0.05, compared with the group of healthy children). The percentage of S. aureus remained high in both groups of operated children.
Local and serum cytokine profiles and antioxidant blood plasma activity in patients with maxillofacial congenital disorders
The analysis of blood cytokines indicated that in the group of patients with CLP, the levels of IL-1β remained above the norm after an initial postoperative increase for a longer time, compared with CL children, and normalized only by day 10 after the surgery vs. day 5 in CL children (Table 2). The difference was most likely due to a larger volume of the surgical intervention in lip and palate plastic surgery.
Table 2. Serum levels of IL-1β in children with maxillofacial congenital disorders before and after surgery, pg/mL±SD
|
Patient groups |
Observation period, days |
||||
|
Before surgery |
1 |
3 |
5 |
10 |
|
|
Children with CL |
13.0±3.0 |
118.0±5.01 |
17.5±4.51 |
14.0±3.0 |
14.0±2.0 |
|
Children with CLP |
13.0±3.0 |
23.0±3.01,2 |
23.5±1.51 |
20.5±2.51 |
18.5±1.53 |
|
Healthy children (control) |
15.0±5.0 |
NA |
NA |
NA |
NA |
1 p<0.05 as compared with control group (healthy children); 2 p<0.05 CL vs. CLP groups; 3 p<0.05 as compared with previous time point (day). NA, not applicable; CL, children with unilateral congenital cleft of upper lip; CLP, children with unilateral congenital cleft of upper lip and palate.
The levels of anti-inflammatory cytokine interleukin-10 (IL-10), which is a major regulator of innate immunity cell activity, exhibited a different trend: after an initial drop in both groups on days 1 and 3 in postoperative period, its levels grew back to initial (i.e., preoperative) values on days 5 and 10 (Table 3).
Table 3. Serum levels of IL-10 in children with maxillofacial congenital disorders in dynamics, before and after surgery, pg/mL±SD
|
Patient groups |
Observation period, days |
||||
|
Before surgery |
1 |
3 |
5 |
10 |
|
|
Children with CL |
10.5±2.5 |
8.5±2.51 |
10.5±2.51 |
10.0±3.0 |
10.0±2.0 |
|
Children with CLP |
10.0±1.0 |
5.0±3.01 |
7.5±1.51, 2 |
9.5±2.5 |
9.5±1.5 |
|
Healthy children (control) |
10.0±2.0 |
NA |
NA |
NA |
NA |
1 p<0.05 as compared with control group (healthy children); 2 p<0.05 CL vs. CLP groups; 3 p<0.05 as compared with previous time point (day). NA, not applicable; CL, children with unilateral congenital cleft of upper lip; CLP, children with unilateral congenital cleft of upper lip and palate.
The local concentrations of proinflammatory cytokine IL-1β increased significantly in the early postoperative period (Figure 2). However, before surgery, local levels of IL-1β were significantly higher than those in healthy patients (p<0.05).
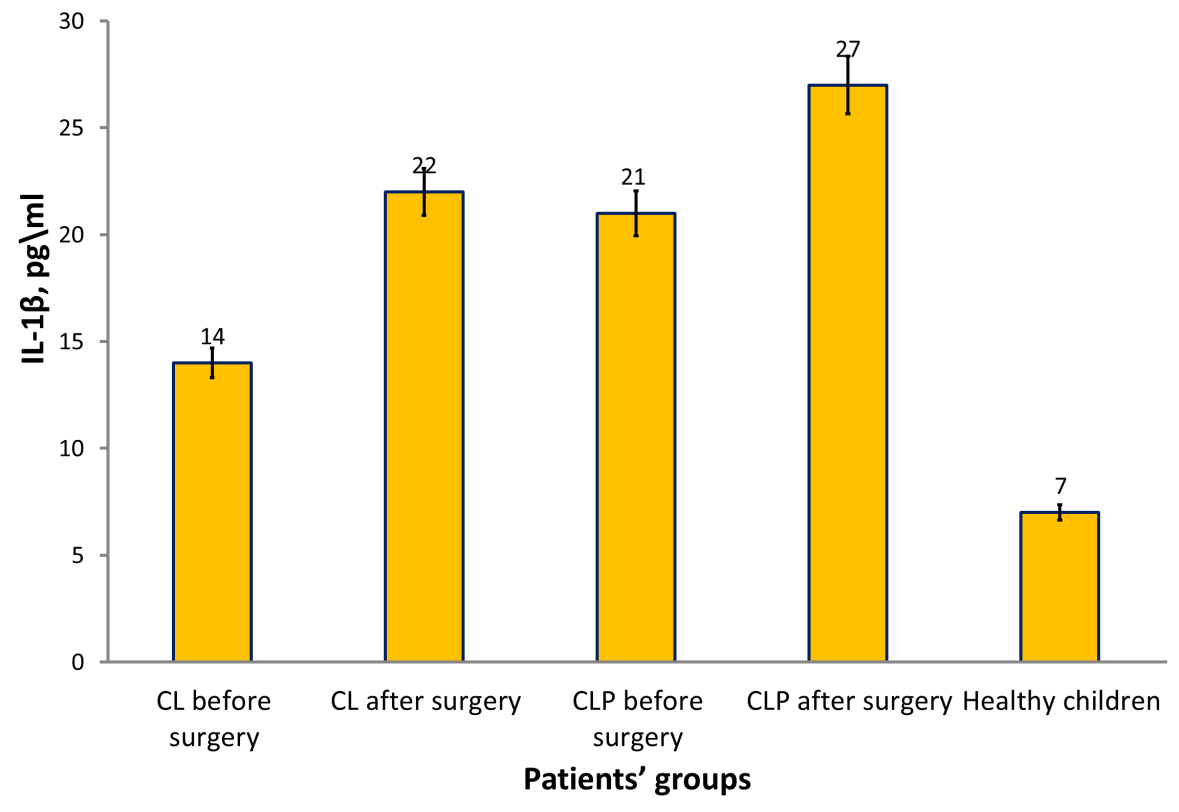
Figure 2. Total viable counts of culturable microbiota of oral, nasal and pharyngeal mucosae in children with CL and CLP in preoperative and postoperative periods. The numbers indicate means of IL-1β concentration within each group and location. Error bars represent confidence intervals. CL, children with unilateral congenital cleft of upper lip; CLP, children with unilateral congenital cleft of upper lip and palate.
Blood plasma antioxidant activity decreased below normal values in the group of patients on days 5-10 after the surgical intervention of cheilorhinoplasty (p<0.05) (Table 4).
Table 4. Levels of blood plasma antioxidant activity in children with congenital disorders of maxillofacial region before and after surgery, %
|
Patient groups |
Observation period, days |
||||
|
Before surgery |
1 |
3 |
5 |
10 |
|
|
Children with CL |
50.0±6.0 |
62.0±3.01 |
59.0±6.0 |
55.0±6.0 |
51.0±6.0 |
|
Children with CLP |
53.0±5.0 |
65.0±2.01 |
62.0±6.01 |
48.0±4.01, 2 |
47.0±5.01 |
|
Healthy children (control) |
55.0±2.0 |
NA |
NA |
NA |
NA |
1 p<0.05 as compared with control group (healthy children); 2 p<0.05 CL vs. CLP groups; 3 p<0.05 as compared with previous time point (day). NA, not applicable; CL, children with unilateral congenital cleft of upper lip; CLP, children with unilateral congenital cleft of upper lip and palate.
An increased antioxidant capacity was found in blood plasma of CL and CLP patients, as compared with healthy children, on day 1 on the postoperative period (Table 4). However, on days 5-7 after the surgery, antioxidant capacity of plasma in the group of patients with more severe defect (CLP) was below normal, which may imply the lack of a compensatory increase of anti-radical enzymes.
Discussion
Preoperative condition of oral, nasal and pharyngeal mucosae directly affects the surgery outcome [9, 12, 33]. Therefore, the quantitative and qualitative composition of microbiota can be considered as one of the major factors influencing a wound healing process. In regard to this, we examined culturable aerobic and facultative microbiota of mucosal surfaces of oronasopharyngeal region, as well as the parameters of pro- and anti-inflammatory immunity and indices of antioxidant activity in CL and CLP patients before and after the surgery. Our findings indicated that children with CLP, but not with CL, had higher mucosal microbial colonization of oropharyngeal region, compared with healthy children. This finding was consistent with the literature data [24, 26, 32]. Hence, we can confirm the severity of congenital disorder of the maxillofacial region that directly affects the state of local microbiota [26, 34].
Continuous postoperative presence of microorganisms with high persistent abilities, such as S. aureus, in our patients may indicate their contamination from parents and/or because of inadequate hygiene [29]. High prevalence of S. aureus and significantly higher levels of microbial colonization of mucosae in children, who underwent the surgery for CLP, suggest an involvement of other systemic and local factors, such as mucosal dryness and reduction in local immunological reactivity, which could make the eradication of a pathogen (e.g., S. aureus), rather difficult [29, 34].
As far as we know, ours is the first study that combined microbiological, immunological and biophysical methods to establish the causes for postoperative complications in children with CL and CLP. Our results indicate that during postoperative period, microbiological parameters partially normalize in CL, but not in CLP patients. However, S. aureus occurrence remained high. Moreover, C. albicans were isolated from three patients implying the condition of local dysbiosis.
The markers of the body’s response to operative trauma include blood and tissue levels of free radicals, specifically, production of free oxygen and nitrogen species by phagocytic cells, as well as the antioxidant capacity of tissues and blood plasma [35]. Reactive oxygen species and nitric oxide are potent bactericidal agents protecting a host from infectious agents, including the situation when normal physical barriers are damaged during the surgery [36].
The results of our study indicated that reactive oxygen species were released during the active phase of wound healing process. However, on days 5-7, the antioxidant capacity of plasma in CLP patients was below normal, which presumes the deficiency of compensatory increase in the production of anti-radical enzymes. It is known that the elevated concentrations of free oxygen and nitrogen radicals can interfere with wound healing due to the inhibition of collagenase activity [37, 38]. The expression of collagenase in fibroblasts of hypertrophic scars is downregulated, which results in a reduced collagen degradation and, therefore, in connective tissue remodeling, along with postoperative complications [39].
Conclusion
In children with CLP, the total microbial counts and the percentage of S. aureus on mucous membranes of the mouth, pharynx and nose were significantly higher than those in healthy children of the age-matching group. Prior to the surgery, the local levels of IL-1β were significantly higher than those found in healthy individuals, which was the sign of proinflammatory nature of tissues. Blood plasma antioxidant activity after surgery declined below normal values in the group of patients after cheilorhinoplasty, which indicated the deficiency of compensatory increase in the production of anti-radical enzymes. The study showed the need for preoperative eradication of such potential pathogens as S. aureus, Klebsiella spp., Candida spp., and Streptococcus spp., preferably, via using non-antibiotic approaches, such as probiotics and phage therapy, as well as supportive integrative therapy (e.g., using antioxidants).
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with 1964 Declaration of Helsinki and its later amendments, or comparable ethical standards.
Conflict of Interest
The authors declare no conflicts of interest.
- Matthews JL, Oddone-Paolucci E, Harrop RA. The epidemiology of cleft lip and palate in Canada, 1998 to 2007. Cleft Palate Craniofac J 2015; 52(4): 417–424. https://doi.org/10.1597/14-047.
- Alonso RRH, Brigetty GPS. Analysis of the prevalence and incidence of cleft lip and palate in Colombia. Cleft Palate Craniofac J 2020; 57(5): 552-559. https://doi.org/10.1177/1055665619886455.
- Nicholls W, Harper C, Robinson S. Data linkage: Cleft live-birth prevalence and hospitalizations in Western Australia: 1980 to 2016. Cleft Palate Craniofac J 2020; 57(10): 1155-1165. https://doi.org/10.1177/1055665620943423.
- Leslie EJ, Carlson JC, Shaffer JR, Feingold E, Wehby G, Laurie CA, et al. A multi-ethnic genome-wide association study identifies novel loci for non-syndromic cleft lip with or without cleft palate on 2p24.2, 17q23 and 19q13. Hum Mol Genet 2016; 25(13): 2862-2872. https://doi.org/10.1093/hmg/ddw104.
- Bilińska M, Osmola K. Cleft lip and palate – risk factors, prenatal diagnosis, and health consequences. Ginekol Pol 2015; 86(11): 862-866. Polish. https://doi.org/10.17772/gp/60371.
- Murray JC. Gene/environment causes of cleft lip and/or palate. Clin Genet 2002; 61(4): 248-256. https://doi.org/10.1034/j.1399-0004.2002.610402.x.
- Tovani-Palone MR, Datta D. Problemas psicológicos y fisura de labio y/o paladar. Rev Fac Cien Med Univ Nac Cordoba 2019; 76(4): 264. https://doi.org/10.31053/1853.0605.v76.n4.23136.
- Kapp-Simon KA. Psychological issues in cleft lip and palate. Clin Plast Surg 2004; 31(2): 347-352. https://doi.org/10.1016/S0094-1298(03)00134-2.
- Hwang DS, Choi HS, Kim UK, Song JM. Complications following orthognathic surgery for patients with cleft lip/palate. J Craniofac Surg 2019; 30(6): 1815-1819. https://doi.org/10.1097/SCS.0000000000005536.
- Rossell-Perry P. Primary cleft rhinoplasty: Surgical outcomes and complications using three techniques for unilateral cleft lip nose repair. J Craniofac Surg 2020; 31(6): 1521-1525. https://doi.org/10.1097/scs.0000000000006043.
- Chauhan JS, Sharma S, Bandi N. Secondary correction of premaxilla in bilateral cleft lip and palate with lag-screw fixation. Br J Oral Maxillofac Surg 2020; 58(9): 1123-1127. https://doi.org/10.1016/j.bjoms.2020.06.013.
- Bennaceur S, Touré R, André CV, Guenane Y, Teissiier N. Secondary cheiloplasty in the treatment of cleft lip and palates. Ann Chir Plast Esthet 2019; 64(5-6): 413-431. French. https://doi.org/10.1016/j.anplas.2019.07.008.
- Kusnadi A, Park SH, Yuan R, Pannellini T, Giannopoulou E, Oliver D, et al. The cytokine TNF promotes transcription factor SREBP activity and binding to inflammatory genes to activate macrophages and limit tissue repair. Immunity 2019; 51(2): 241-257.e9. https://doi.org/10.1016/j.immuni.2019.06.005.
- Menges P, Kessler W, Kloecker C, Feuerherd M, Gaubert S, Diedrich S, et al. Surgical trauma-induced immunosuppression in cancer: Recent advances and the potential therapies. Eur Surg Res 2012; 48(4): 180-186. https://doi.org/10.1159/000338196.
- Menges P, van der Linde J, Hegenbart A, Heidecke CD, Maier S. Characterisation of Postoperative Immune Suppression by Validated Parameters in Visceral Surgery. Zentralbl Chir 2016; 141(1): 68-74. German. https://doi.org/10.1055/s-0032-1328349.
- Romeo C, Cruccetti A, Turiaco A, Impellizzeri P, Turiaco N, Di Bella C, et al. Monocyte and neutrophil activity after minor surgical stress. J Pediatr Surg 2002; 37(5): 741-744. https://doi.org/10.1053/jpsu.2002.32268.
- Zhang T, Wang XF, Wang ZC, Lou D, Fang QQ, Hu YY, et al. Current potential therapeutic strategies targeting the TGF-beta/Smad signaling pathway to attenuate keloid and hypertrophic scar formation. Biomed Pharmacother 2020; 129: 110287. https://doi.org/10.1016/j.biopha.2020.110287.
- Mantovani A, Dejana E. Cytokines as communication signals between leukocytes and endothelial cells. Immunol Today 1989; 10(11): 370-375. https://doi.org/1016/0167-5699(89)90270-3.
- Sies H. Oxidative stress: a concept in redox biology and medicine. Redox Biol 2015; 4: 180-183. https://doi.org/10.1016/j.redox.2015.01.002.
- Jones DP. Radical-free biology of oxidative stress. Am J Physiol Cell Physiol 2008; 295(4): C849-C868. https://doi.org/10.1152/ajpcell.00283.2008.
- Curi R, Levada-Pires AC, Silva EBD, Poma SO, Zambonatto RF, Domenech P, et al. The critical role of cell metabolism for essential neutrophil functions. Cell Physiol Biochem 2020; 54(4): 629-647. https://doi.org/10.33594/000000245.
- Berman B, Maderal A, Raphael B. Keloids and hypertrophic scars: Pathophysiology, classification, and treatment. Dermatol Surg 2017; 43 Suppl 1: S3-S18. https://doi.org/10.1097/DSS.0000000000000819.
- Lee HJ, Jang YJ. Recent understandings of biology, prophylaxis and treatment strategies for hypertrophic scars and keloids. Int J Mol Sci 2018; 19(3): 711. https://doi.org/10.3390/ijms19030711.
- Zhang T, Wang XF, Wang ZC, Lou D, Fang QQ, Hu YY, et al. Current potential therapeutic strategies targeting the TGF-beta/Smad signaling pathway to attenuate keloid and hypertrophic scar formation. Biomed Pharmacother 2020; 129: 110287. https://doi.org/10.1016/j.biopha.2020.110287.
- Chen H, Xu Y, Yang G, Zhang Q, Huang X, Yu L, Dong X. Mast cell chymase promotes hypertrophic scar fibroblast proliferation and collagen synthesis by activating TGF-beta1/Smads signaling pathway. Exp Ther Med 2017; 14(5): 4438-4442. https://doi.org/10.3892/etm.2017.5082.
- Machorowska-Pieniążek A, Mertas A, Skucha-Nowak M, Tanasiewicz M, Morawiec T. A Comparative study of oral microbiota in infants with complete cleft lip and palate or cleft soft palate. Biomed Res Int 2017; 2017: 1460243. https://doi.org/10.1155/2017/1460243.
- Bariar LM, Ahmad I, Sharma SC. An otorhinological study of patients with cleft lip and palate. Indian J Otolaryngol Head Neck Surg 2001; 53(3): 250-252. https://doi.org/10.1007/BF03028569.
- Aras I, Dogan S. Comparative evaluation of the pharyngeal airways and related soft tissues of unilateral and bilateral cleft lip and palate patients with the noncleft individuals. Cleft Palate Craniofac J 2017; 54(1): 53-59. https://doi.org/10.1597/15-055.
- Cocco JF, Antonetti JW, Burns JL, Heggers JP, Blackwell SJ. Characterization of the nasal, sublingual, and oropharyngeal mucosa microbiota in cleft lip and palate individuals before and after surgical repair. Cleft Palate Craniofac J 2010; 47(2): 151-155. https://doi.org/10.1597/08-187_1.
- Kharaeva ZF, Zhanimova LR, Mustafaev MSh, De Luca C, Mayer W, Chung Sheun Thai J, et al. Effects of standardized fermented papaya gel on clinical symptoms, inflammatory cytokines, and nitric oxide metabolites in patients with chronic periodontitis: An open randomised clinical study. Mediators Inflamm 2016; 2016: 9379840. https://doi.org/10.1155/2016/9379840.
- Vasiljeva OV, Lyubitsky OB, Klebanov GI, Vladimirov YuA. Effect of antioxidants on the kinetics of chain lipid peroxidation in liposomes. Membr Cell Biol 1998; 12(2): 223-231. https://pubmed.ncbi.nlm.nih.gov/9879545.
- Funahashi K, Shiba T, Watanabe T, Muramoto K, Takeuchi Y, Ogawa T, et al. Functional dysbiosis within dental plaque microbiota in cleft lip and palate patients. Prog Orthod 2019; 20(1): 11. https://doi.org/10.1186/s40510-019-0265-1.
- Rossell-Perry P. Primary cleft rhinoplasty: Surgical outcomes and complications using three techniques for unilateral cleft lip nose repair. J Craniofac Surg 2020; 31(6): 1521-1525. https://doi.org/10.1097/SCS.0000000000006043.
- Ruegg TA, Cooper ME, Leslie EJ, Ford MD, Wehby GL, Deleyiannis FW, et al. Ear infection in isolated cleft lip: Etiological implications. Cleft Palate Craniofac J 2017; 54(2): 189-192. https://doi.org/10.1597/15-010.
- Sies H. Oxidative stress: A concept in redox biology and medicine. Redox Biol 2015; 4: 180-183. https://doi.org/10.1016/j.redox.2015.01.002.
- Yang S, Lian G. ROS and diseases: Role in metabolism and energy supply. Mol Cell Biochem 2020; 467(1-2): 1-12. https://doi.org/10.1007/s11010-019-03667-9.
- Yu H, Huang J, Wang S, Zhao G, Jiao X, Zhu L. Overexpression of Smad7 suppressed ROS/MMP9-dependent collagen synthesis through regulation of heme oxygenase-1. Mol Biol Rep 2013; 40(9): 5307-5014. https://doi.org/10.1007/s11033-013-2631-2.
- Saito-Takatsuji H, Yoshitomi Y, Ishigaki Y, Yamamoto S, Numata N, Sakai Y, et al. Protective effects of collagen tripeptides in human aortic endothelial cells by restoring ROS-induced transcriptional repression. Nutrients 2021;13(7):2226. https://doi.org/10.3390/nu13072226.
- Huo Y, Qiu W-Ya, Pan Q, Yao Yu-F, Xing K, Lou MF. Reactive oxygen species (ROS) are essential mediators in epidermal growth factor (EGF)-stimulated corneal epithelial cell proliferation, adhesion, migration, and wound healing. Exp Eye Res 2009; 89(6): 876-886. https://doi.org/10.1016/j.exer.2009.07.012.20.
Received 1 October 2021, Revised 30 November 2021, Accepted 10 December 2021
© 2021, Russian Open Medical Journal
Correspondence to Zaira F. Kharaeva. Address: Department of Microbiology, Virology, and Immunology, School of Medicine, Kabardino-Balkarian State University, 5 Gorky St., Nalchik 360000, Kabardino-Balkaria, Russia. Phone: +79287089166. E-mail: irafe@yandex.ru.
Selected papers from the International Scientific and Practical Conference “Basic Science for Practical Medicine – 2021”, 15–18 September 2021, Elbrus v., Russia, http://uniid.kbsu.ru/medicine2021