Introduction
The mortality in traumas of parenchymatous organs remains high, reaching 15-35% [1]. Hemoperitoneum is the main cause of unfavorable outcomes in hepatic and splenic traumas. Hence, the selection of adequate arrest of bleeding and timely surgical intervention are of utmost importance [2]. The survival of patients operated within less than 2 hours of the parenchymatous organ trauma is 90%; in those operated within 6–12 hours is 25%; and in patients undergoing surgical treatment more than 12 hours after the trauma is haphazard [3, 4].
All aforementioned factors lead to technical difficulties during surgical interventions as well. Surgical tactics in hepatic injuries is defined by the trauma character and is aimed primarily at effective hemostasis [5]. However, there is no description of the optimal intraoperative tactics in open access publications concerning the maneuvers necessary for temporary or complete hemostasis, as well as regarding the choice of intervention versus injury severity. The latter is essential for the individual approach to treating injuries and stopping bleeding, because the techniques used for both are quite variable [6, 7]. Advancements of hemostatic methods, selection of tactics in splenic or hepatic traumas and subsequent surgeries are rather important since, despite significant surgical achievements, mortality in traumas of parenchymatous organs remains quite high [8, 9].
The use of local hemostatic agents (LHA) optimizes surgical techniques via shortening interventions. The analysis of published data regarding practical use of different LHA (solutions, gels, pastes, films, foams, as well as fabric and non-fabric materials) demonstrated that foams were the most effective agents due to their capillary and porous structure [10, 11].
Currently, there are many LHA based on various organic and inorganic substances, and each of those has its own advantages and drawbacks. An important criterion for their use is their bioavailability and mild responses of human tissues to their implantation [12]. A significant number of publications was devoted to issues of tissue responses in traumatized organs to LHA. These studies were usually performed on laboratory animals, such as rats, rabbits, and miniature pigs. Apart from animal species diversity, experimental models for specific organ traumas were standardized as well, which makes it difficult to compare data obtained in different studies [13]. Despite that, domestic and foreign authors presented the results of studying liver tissue responses to applying various types of hemostatic agents with different mechanisms of action: CeloxТМ gauze hemostat (chitosan); QuikClot and Hemostop (synthetic zeolite); WoundStat (smectite); Surgicel Nu-knit (oxidized and reduced cellulose); and TachoComb (collagen). In each case, author-selected criteria were used for evaluating the severity of animal tissue response to LHA (presence of necrotic foci, changes in hepatocyte structure or the ratio of cellular parenchymal elements, cell indices, etc.) [14, 15].
However, among open access publications, those that are based on the studies involving original hemostatic material samples developed by scientific groups with the addition of agents, characterized by a significant hemostatic effect and used in clinical practice, are of utmost importance, because of high relevance of searching for the most promising materials for LHA manufacturing.
Study objective: to evaluate changes in liver tissues after simulated injury and use of novel hemostatic agents (containing tranexamic acid) in the course of in vivo experiment.
Material and Methods
Study materials
The study materials included samples of various local hemostatic agents (LHA). Group 1 included patients subjected to TachoComb® collagen plate of the following composition: collagen from equine tendons; riboflavin; lyophilized human fibrinogen; thrombin; aprotinin; manufactured by Takeda, Linz, Austria). Group 2 comprised patients subjected to experimental samples based on 4% sodium carboxymethyl cellulose (Na-CMC), developed by a group of authors and manufactured in the scientific laboratory of Lintex LLC, Saint-Petersburg, Russia. Group 3 encompassed patients subjected to 4% Na-CMC + tranexamic acid (TA) in the amount of 3% of the polymer weight.
Laboratory animals
The study was performed on 30 male rabbits of the Soviet chinchilla breed (10 animals per group) weighing 2.5-3 kg each. All applicable international and Russian laboratory animal welfare standards were followed (under the supervision of the Regional Ethics Committee at Kursk State Medical University (KSMU), Ministry of Healthcare of the Russian Federation).
Modeling liver trauma
Anesthetic support presumed employing inhalation mask anesthesia (isoflurane concentration in the inhaled gas mixture of 3%; air flow of 0.8 L/min). In sterile conditions of the operation unit at the Laboratory of Experimental Surgery and Oncology (Scientific Research Institute of Experimental Medicine, KSMU), all animals were placed on the surgical table in the supine position. After surgical field treatment and delimitation, carbon dioxide pneumoperitoneum was applied with subsequent abdominal cavity examination and liver identification. Then two laparoscopic ports (3 mm in diameter) were installed successively. The endoscopic dissector was used to divide the medial lobe of the liver bluntly and cranially at the distance of 5 cm from its edge for the whole depth of the dissector jaw (12 mm); wound edges were stretched apart. A tested sample 1x1 cm in size was placed in the wound and tightly fixed with an instrument (Method of Modeling Laparoscopic Lacerated Liver Wound in Laboratory Animals for The Studies of Hemostatic Materials; Eurasian patent application No. 202000200/25 of July 23, 2020). The animals were sacrificed under anesthesia via cervical dislocation on Day 30 after the surgery.
Morphological and morphometric parameters
Histological specimens were fixed in 10% neutral buffered formalin for 7 days. Using the conventional method, paraffin blocks and microslides were prepared; the latter were stained with hematoxylin and eosin. Morphometric evaluation presumed photographs of microslides made with Leica ScanScope CS2 digital microslide scanner for the light field (manufactured by Leica Biosystems, Wetzlar, Germany), using ×40, ×100, ×200, and ×400 magnification values. Using TopView software (manufactured by ToupTek Photonics, Hangzhou, China), the following parameters were measured on obtained microphotographs: capsule thickness (µm), sizes of hepatocytes and their nuclei (px), number of binuclear hepatocytes, nuclear-cytoplasmic ratio NCR) for hepatocytes (see the formula below), qualitative and quantitative composition of the capsule surrounding the tested sample (number of macrophages, fibroblasts, fibrocytes, leukocytes). NCR was calculated as the ratio of the cell nucleus area to the cytoplasmic area. NCR is considered an important morphological trait allowing to evaluate the level of metabolism in hepatic cells, hence detecting signs of compensatory reactions:
NCR = S hepatocyte nucleus / S hepatocyte cytoplasm,
where: S hepatocyte nucleus is the hepatocyte nucleus area, px; S hepatocyte cytoplasm is the cell (hepatocyte) area, px.
The formular for the cell index (CI), which is the ratio of resident cells to non-resident cells, is as follows:
CI = resident cells / non-resident cells,
where: resident cells include the total number of macrophages, fibroblasts, and fibrocytes; non-resident cells include the total number of leukocytes in the cellular capsule layer.
CI values below 1 were implying that inflammatory changes typical for the first phase of the wound healing predominated; CI values over 1 were suggesting that reparative trends typical for the second phase (sensu M.I. Kuzin) were predominant.
Statistical data processing
Preliminary data processing demonstrated they did not comply with the Gaussian distribution. Accordingly, the following descriptive statistics parameters were used: median (Me), 25% and 75% quartiles: (Q25, Q75). Due to small sample sizes in experimental study groups (n˂30) and specificity of data distribution, we used nonparametric Mann-Whitney U test as the main method to identify the statistical significance of differences. When evaluating the significance of differences, the 5% error (p≤0.05) was considered acceptable for medical and biological experiments. The Statistica software package (version 10.0) was employed for data processing.
Results
Description of histology slides
When studying the liver fragment after using the TachoComb collagen plate (on day 30 after surgery), distinct necrotic zone was detected in the trauma location around the remaining material fragments; this zone was separated from the hepatic parenchyma with a sufficiently wide (0.51 mm) fibrous capsule (Figure 1) (Table 1). Material sequestration with exudative effusion was observed in the center of the zone, and the collagen formation process was thereby spreading to adjacent hepatic lobules with septal fibrosis.

Figure 1. Micrograph of the liver fragment after applying TachoComb collagen plate (on postoperative day 30). The boundary between liver parenchyma and preserved fragments of the tested sample. Hematoxylin and eosin staining, magnification ×100.
Table 1. Thickness of the capsule surrounding tested samples, Me [25; 75]
|
Groups |
Capsule width, mm |
|
TachoComb |
0.51 (0.45, 0.67) |
|
Na-CMC |
0.16 (0.15, 0.16) |
|
Na-CMC + tranexamic acid |
0.14 (0.13, 0.16) |
|
p1 |
0.0002* |
|
p2 |
0.0002* |
|
p3 |
0.344 |
* statistically significant changes (p≤0.05); p1 – significance level for TachoComb group vs. Na-CMC group; p2 – significance level for TachoComb group vs. Na-CMC + tranexamic acid group; p3 – significance level for Na-CMC group vs. Na-CMC + tranexamic acid group. Data are presented as median with low and upper quartiles – Me (Q25, Q75).
The capsule around sample fragments had a double-layered structure. The peripheral layer consisted of more mature, ordered collagen fibers. Cellular composition was represented predominantly by fibroblasts with inclusions of lymphocytes and segmented leukocytes (Table 2). In the interior capsule layer, collagen fibers were thinner, and they were loosely distributed, with polymorphonuclear infiltration. In adjacent liver parenchyma, we observed focal decomplexation of hepatic laminae with mild edema (Figure 2).
Table 2. Morphometric parameters of liver parenchyma in studied groups, Me [25; 75]
|
Groups |
Index |
|||
|
Number of binuclear hepatocytes |
Hepatocyte area, px |
Nucleus area, px |
Nuclear-cytoplasmic ratio |
|
|
TachoComb |
15 (15, 16) |
190.28 (187.52, 193.10) |
169.9 (154.4, 179.9) |
0.89 (0.82, 0.95) |
|
Na-CMC |
27 (26, 28) |
197.11 (191.73, 201.23) |
165.1 (158.1, 170.7) |
0.84 (0.81, 0.87) |
|
Na-CMC + tranexamic acid |
22 (21, 23) |
191.03 (180.97, 201.72) |
147.8 (134.7, 159.3) |
0.76 (0.72, 0.83) |
|
p1 |
0.0002* |
0.001* |
0.225 |
0.021* |
|
p2 |
0.0002* |
0.787 |
0.000* |
0.000* |
|
p3 |
0.0002* |
0.053 |
0.000* |
0.003* |
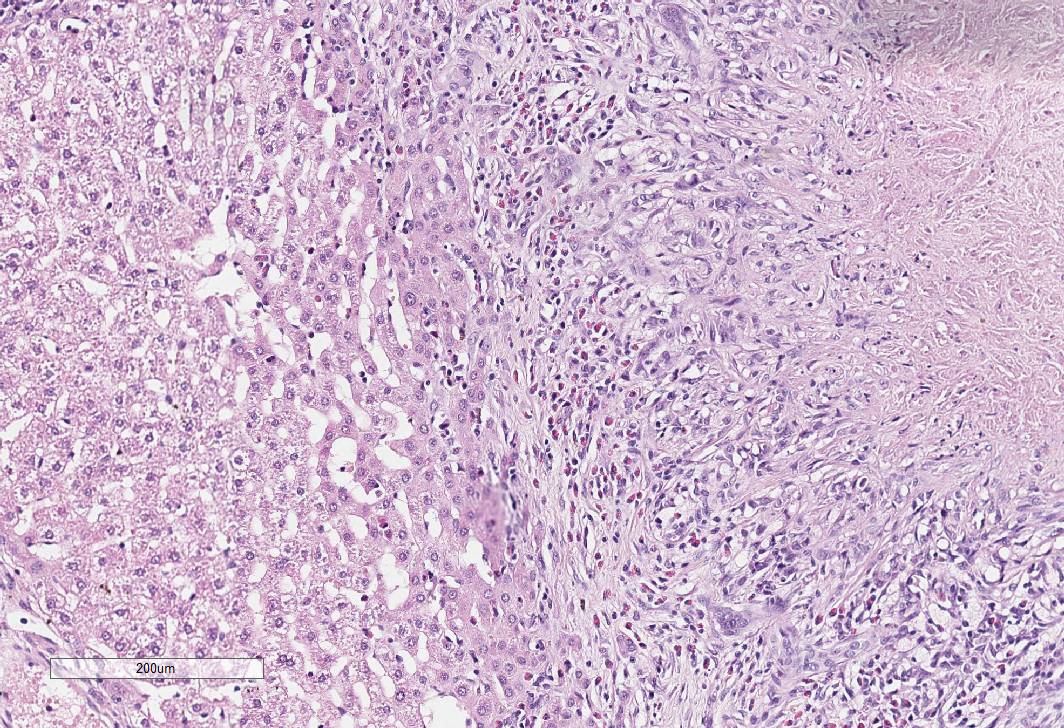
Figure 2. Micrograph of the liver fragment after applying TachoComb hemostatic sponge (on postoperative day 30). Necrobiotic changes in adjacent liver parenchyma. Hematoxylin and eosin staining, magnification ×200.
In general, parenchyma preserved laminar structure with lobule formation. However, it should be noted that hepatocytes were also changing with the development of granular dystrophy. The vasculature demonstrated venous lumen dilation and perivascular edema. Bile ducts and arterial vessels were of normal morphological structure.
When studying the liver fragment after using the hemostatic sponge based on Na-CMC with tranexamic acid (Group 3), we observed the overgrowth of fibrous tissue with encapsulation of the used material. The capsule width was thinner than in Group 1 (0.14 mm). The fibrous tissue grew between polymer fibers, but did not spread deeper into the liver parenchyma.
Moderate lymphocytic infiltration was preserved in the central part around sample residues. Along the periphery, the capsule consisted entirely of fibers tightly adjacent to each other. From the outer part, bile ducts grew into the capsule. The adjacent parenchyma preserved its laminar structure. Compared with Group 1, hepatocytes also had signs of granular dystrophy (Figure 3).

Figure 3. Micrograph of the liver fragment after applying hemostatic sponge based on Na-CMC + tranexamic acid (on postoperative day 14). Signs of granular hepatocyte degeneration in adjacent liver parenchyma. Hematoxylin and eosin staining, magnification ×400.
When studying the liver fragment from Group 2, we detected a thin film of the fibrous tissue that surrounded the tested material circularly, forming the mature fibrous capsule. Inflammatory infiltration was absent. The fibrous capsule thickness in this group (0.156 mm) was significantly less, compared with Groups 1 and 3 using other materials (Figure 4).
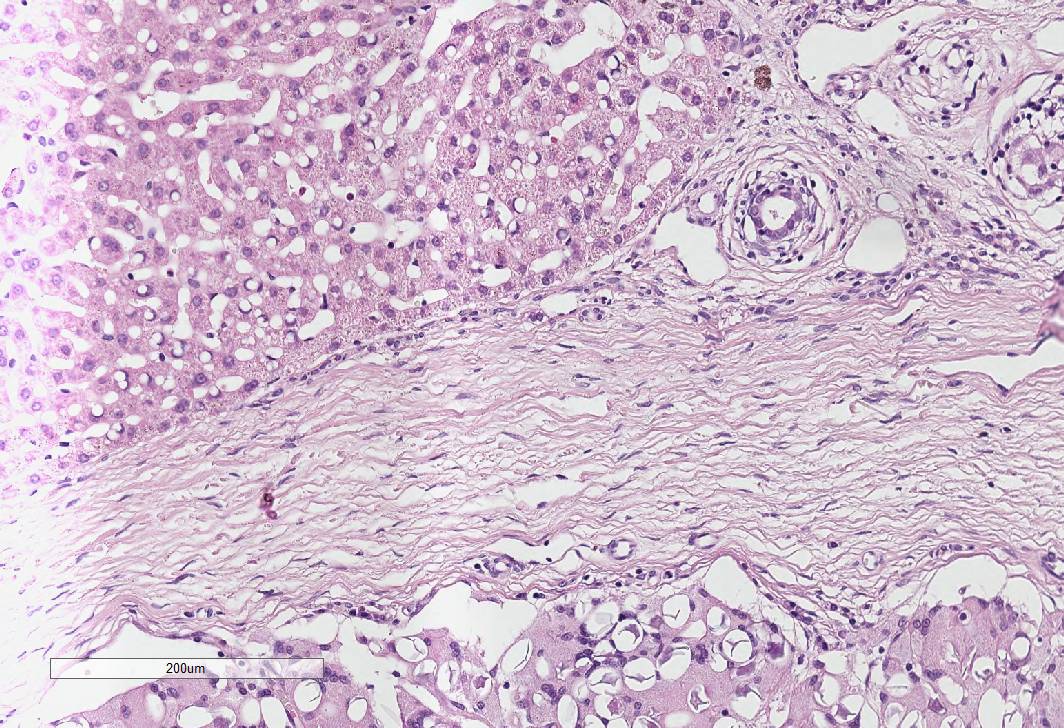
Figure 4. Micrograph of the liver fragment after applying hemostatic sponge based on Na-CMC (on postoperative day 30). Fibrous capsule around sample fragments. Hematoxylin and eosin staining, magnification ×400.
In adjacent areas the parenchyma had signs of mild edema and moderately significant perivascular lymphocytic infiltration. Compared with other groups, the thickness of the fibrous liver capsule was mildly increased.
Various surgical manipulations in hepatic tissues definitely lead to morphofunctional changes in the liver parenchyma. To evaluate them, NCR and the number of binuclear hepatocytes were calculated and analyzed (Table 2). Changes in the number of polyploid, and particularly, binuclear cells confirmed the functional organ strain and significant course of regenerative processes in the traumatized organ.
Morphometric study data
In Group 1, polygonal hepatocytes contained one or two oval nuclei, with occasional hypertrophic hepatocytes. A larger number of dividing cells with incomplete karyo- and cytokinesis was observed. The NCR was higher (0.89), compared with foams based on Na-CMC with or without tranexamic acid (0.76 and 0.84, respectively) (Table 2) (p≤0.05). This could be related to more significant dystrophic changes in hepatocytes, with increased cytoplasmic and total cell areas.
In Groups 2 and 3, hepatocytes had a tetra- or pentagonal (sometimes oval or elongated) shape, their cytoplasm was uniformly oxyphilic. The nucleus, usually located in the center of the cell, had a rounded or oval shape and was stained in a basophilic way. The majority of hepatocytes contained a single nucleus, however binuclear cells were also detected. It should be noted that these groups demonstrated the increased number of binuclear hepatocytes, compared with the TachoComb group (27 and 22, respectively), which has also confirmed the active course of regenerative processes. With that, no pathologically changed hepatocytes were detected in the preserved liver parenchyma.
We also considered such quantitative parameters as the number of fibroblastic cells and phagocytic cells (macrophages, leukocytes), which allowed analyzing the structure of the periprosthetic capsule and the prominence of its layers. According to obtained data (Table 3), it should be noted that the largest number of fibroblastic cells was observed in the capsule surrounding materials in Group 3. The number of fibroblasts in this group exceeded the values of other groups by 4.5 (Group 2) and by 7.5 (Group 1) (p≤0.05). The number of fibrocytes in Group 3 was also significantly greater than in Group 2 (by 8.5) and Group 1 (by 10) (p≤0.05). When considering the number of inflammatory cells, lymphocytes were predominant in Group 2 (p≤0.05): their number prevailed over Group 1 by 1.5 and over Group 3 by 4.5. However, the number of macrophages in Group 1 was 3 more than in Group 2 and 6 more than in Group 3 (p≤0.05). The number of neutrophils, eosinophils, and monocytes prevailed in Group 1. The number of neutrophils in Group 1 was higher by 1.5 and 4.5 than in Groups 2 and 3, respectively, while the number of eosinophils was higher by 1 and 2.5. The number of monocytes in Group 1 exceeded that in Groups 2 and 3 by 1.5 (p≤0.05).
Table 3. Cellular composition of the capsule surrounding tested samples, Me [25; 75]
|
Groups |
Cells |
||||||
|
Fibroblasts |
Fibrocytes |
Lymphocytes |
Macrophages |
Neutrophils |
Eosinophils |
Monocytes |
|
|
TachoComb |
25 (24, 26) |
29.5 (29, 30) |
8 (8, 9) |
15 (14, 16) |
9.5 (8, 10) |
7.5 (6, 8) |
5.5 (4, 6) |
|
Na-CMC |
28 (28, 28) |
31 (30, 32) |
9.5 (9, 11) |
12 (12, 13) |
8 (7, 9) |
6.5 (6, 7) |
4 (4, 6) |
|
Na-CMC + tranexamic acid |
32.5 (32, 34) |
39.5 (38, 40) |
5 (4, 6) |
9 (9, 10) |
5 (4, 6) |
5 (4, 6) |
4 (3, 4) |
|
p1 |
0.0004* |
0.009* |
0.039* |
0.0003* |
0.031* |
0.131 |
0.289 |
|
p2 |
0.0002* |
0.0002* |
0.0002* |
0.0002* |
0.0002* |
0.0007* |
0.010* |
|
p3 |
0.0001* |
0.0002* |
0.0002* |
0.0003* |
0.0003* |
0.014* |
0.104 |
According to CI calculations (Table 4) performed to objectively compare the response of laboratory animal tissues to the tested samples, its largest value was observed in Group 3 (4.26). Its values in other groups were significantly lower: 1.74 times smaller (Group 1) and 1.69 times smaller (Group 2). Hence, we conclude about the significant predominance of reparative processes in Group 3, compared with other groups.
Table 4. Results of cell index (CI) calculation in study groups, Me [25; 75]
|
Index |
Group |
||
|
TachoComb |
Na-CMC (unpressed) |
Na-CMC + tranexamic acid (unpressed) |
|
|
CI |
2.448 (2.030, 2.571) |
2.510 (2.330, 2.704) |
4.263 (4.263, 4.555) |
|
p |
p1=0.106 |
p2=0.0002* |
p3=0.0002* |
Discussion
One of the major current issues in abdominal surgery is the search for reliable and non-traumatic methods of stopping bleeding caused by traumas of parenchymatous abdominal organs [12]. In such cases, hemostasis efficacy and safety are the main factors that matter in preserving the patient’s life and in designing further postoperative course of healing. Conventionally used approaches to the arrest of bleeding (hemostatic sutures, electro coagulation, spray coagulation, etc.) are, in fact, invasive, since they cause injuries to the organ tissues [15].
LHA represent the opposite, non-invasive (non-suture) approach to stopping such bleedings, because they do not traumatize the injured organ due to proper mechanisms of their action [1]. This is the most important advantage of using LHA: there are no organ traumas during the arrest of bleeding and there is much smaller rate of postoperative complications [5]. The action of LHA is based on several components: specifically, their porous structure, biodegradable base (collagen, medical grade gelatin, cellulose derivatives), and the presence of biologically active or medicinal products with various effects (antibacterial, coagulative, etc.) [4].
According to investigators dealing with the issues of development and experimental trials of new LHA samples, the severity of tissue response to LHA implantation depends on material composition and structure. Hence, samples based on polymer fibers of the oxidized cellulose (Surgicel®) are characterized by high pH value, which severely injures liver parenchyma due to the formation of necrotic foci in the perifocal material [11,14]. The main advantage of Surgicel is its high biodegradation rate. However, this agent is hardly an optimal material for hepatic surgery, since it accounts for significant traumatization of injured organ tissues [3]. On the other hand, in the implantation zone, hemostatic agents based on animal collagen (such as TachoComb) cause significant inflammatory reaction due to the chemical structure, while the significant immune response is related to a high concentration of foreign proteins. However, no additional tissue traumas were detected (as was the case with Surgicel), but prolonged inflammation led to slow destruction of the material bed, thereby supporting the course of exudation and proliferation processes [10, 13].
In this study, we presented our experience with the chronic in vivo experiment testing novel LHA samples based on Na-CMC with or without tranexamic acid. Development of these agents was based on the aforementioned data of our Russian and foreign colleagues. This has allowed developing the material possessing advantageous properties of the hemostatic agents already used in clinical practice, but also surpassing them in some features.
Thus, according to the results of the performed morphological study, we revealed that fragments of all tested materials could be identified in the zone of injured liver tissues, despite significant period of time elapsing after the trauma (30 days). The significant borderline zone was also observed, separating LHA materials from the liver parenchyma due to connective tissue growth in the course of the inflammatory reaction. However, the degree of severity of these processes differed among the experimental groups. For example, in the collagen plate group the capsule width was 3.2- and 3.6-fold of its values in Groups 2 and 3. This finding demonstrated indirectly a more prominent course of inflammatory and regenerative processes aimed at limiting the injury zone. This was also confirmed by statistically significant differences in the cellular composition of the capsule: in Groups 2 and 3, fibroblastic cells predominated, and their numbers were higher than in Group 1. The largest CI value was also observed in Group 3, which confirmed the smaller intensity of inflammatory response to the tested sample material (the number of inflammatory cells was smaller than the number of fibroblastic cells).
Conclusion
Our pioneering experience of using LHA, based on Na-CMC with the addition of tranexamic acid, in the chronic in vivo experiment has demonstrated satisfactory results. This finding was supported by less severe inflammatory response of tissues in histological sections, compared with an analog widely used in clinical practice.
Conflict of interest
The authors declare no conflicts of interest.
Compliance with ethical standards
The study was conducted in compliance with the following regulatory acts: Directive 2010/63/EU of the European Parliament and the European Council, On the Protection of Animals Used for Scientific Purposes; Order of the Ministry of Healthcare of the Russian Federation No. 199n of April 01, 2016, On Approving the Rules of Good Laboratory Practice; Order of the Ministry of Healthcare of the USSR No. 755 of August 12, 1977, On Measures for Further Improvement of Organizational Forms oа Studies Using Experimental Animals; etc. Our study has also complied with the principles of 1975 Declaration of Helsinki (1983 revision).
- Lutsevich OE, Grin AA, Bichev AA, Shepelev VV. Features of the application of hemostatic material topical surgery. Moscow Surgical Journal 2016; (3(49)): 12-20. Russian. https://www.elibrary.ru/item.asp?id=28436977.
- Lipatov VA, Kudryavtseva TN, Severinov DA. Application of cellulose derivatives in experimental surgery of parenchymal organs. Science of the young (Eruditio Juvenium) 2020; 8(2): 269-283. Russian. https://doi.org/10.23888/HMJ202082269-283.
- Sadykov RA, Ismailov BA, Kim OV. New film coating based on cellulose derivatives for local hemostasis. Novosti Khirurgii 2019; 27(3): 256-263. Russian. https://doi.org/10.18484/2305-0047.2019.3.256.
- Takagi T, Tsujimoto H, Torii H, Ozamoto Y, Hagiwara A. Two-layer sheet of gelatin: A new topical hemostatic agent. Asian J Surg 2018; 41(2): 124-130. https://doi.org/10.1016/j.asjsur.2016.09.007.
- Zhavoronok IS, Kondratenko GG, Gapanovich VN, Esepkin AV, Karman AD. The arrest of bleeding from the liver parenchyma by using an inorganic hemostatic agents. Novosti Khirurgii 2016; 24(4): 361-367. Russian. https://doi.org/10.18484/2305-0047.2016.4.361.
- Kang BS, Na YC, Jin YW. Comparison of the wound healing effect of cellulose and gelatin: An in vivo study. Arch Plast Surg 2012; 3(4): 317-322. https://doi.org/10.5999/aps.2012.39.4.317.
- Lipatov VA, Lazarenko SV, Sotnikov KA, Severinov DA, Ershov MP. To the issue of methodology of comparative study of the degree of hemostatic activity of topical hemostatic agents. Novosti Khirurgii 2018; 26(1): 81-95. Russian. https://doi.org/10.18484/2305-0047.2018.1.81.
- Zheng C, Zeng Q, Pimpi S, Wu W, Han K, Dong K, Lu T. Research status and development potential of composite hemostatic materials. J Mater Chem B 2020; 25(8): 5395-4410. https://doi.org/10.1039/D0TB00906G.
- Green CS, Bulger EM, Kwan SW. Outcomes and complications of angioembolization for hepatic trauma: A systematic review of the literature. J Trauma Acute Care Surg 2016; 80(3): 529-537. https://doi.org/10.1097/TA.0000000000000942.
- Shukla A, Fang JC, Puranam S, Jensen FR, Hammond PT. Hemostatic multilayer coatings. Adv Mater 2012; 24(4): 492-496. https://doi.org/10.1002/adma.201103794.
- Kaptanoglu L, Kurt N, Sikar HE. Current approach to liver traumas. Int J Surg 2017; 39: 255-259. https://doi.org/10.1016/j.ijsu.2017.02.015.
- Takagi T, Tsujimoto H, Torii H, Ozamoto Y, Hagiwara A. Two-layer sheet of gelatin: A new topical hemostatic agent. Asian J Surg 2018; 41(2): 124-130. https://doi.org/10.1016/j.asjsur.2016.09.007.
- Chen Y, Wu L, Li P, Hao X, Yang X, Xi G, et al. Polysaccharide based hemostatic strategy for ultrarapid hemostasis. Macromol Biosci 2020; 20(4): e1900370. https://doi.org/10.1002/mabi.201900370.
- Arora ND, Varghese R, Pavithran S, Kothandam S. The pressures of Surgicel® in cardiac surgery. Ann Pediatr Cardiol 2015; 8(2): 167-169. https://doi.org/10.4103/0974-2069.157040.
- Wu Z, Zhou W, Deng W, Xu C, Cai Y, Wang X. Antibacterial and hemostatic thiol-modified chitosan-immobilized AgNPs composite sponges. ACS Appl Mater Interfaces 2020; 2(18): 20307-20320. https://doi.org/10.1021/acsami.0c05430.
Received 29 September 2020, Revised 23 August 2021, Accepted 24 January 2022
© 2020, Russian Open Medical Journal
Correspondence to Dmitry A. Severinov. Address: 3 K. Marx St., Kursk 305041, Russia. E-mail: dmitriy.severinov.93@mail.ru.