Introduction
Thermal hand injury (THI) is a severe open injury to superficial and deep tissues of the hand caused by exposure to high temperatures. THI is characterized by different severity grades of damage to the tissues and hand structures, vascular changes, occurrence of local and complex inflammatory response, formation of secondary cicatricial skin changes, as well as of inner tissues, and/or secondary deformation and dysfunction of the hand (up to subsequent disability of the patient) [1]. Children under 5 years of age usually have higher hospitalization and mortality rates caused by thermal injuries. THI constitutes 69.1% of upper limb burn cases among children. The time of exposure to a thermal damaging factor among young children is higher, compared with older children and adolescents, due to the fact that they are not aware of possible consequences THI and, in most cases, cannot independently stop exposure to a damaging thermal factor, if possible at all. This causes a greater severity of THI among young children [2]. The economic burden of THI in children and youths is high, since it includes direct and indirect costs associated with therapeutic and surgical treatment of THI and its consequences, the need for special training of combustiologists, orthopedic traumatologists and/or plastic surgeons, an introduction of modern techniques of reconstructive treatment and rehabilitation as well as innovative technologies. THI is also a substantial financial problem for the healthcare system due to a long period of recovery and rehabilitation.
An average cost of treating one completed case of THI in the United States is $2,810 and an average cost of a bed-day is $195. In the Russian Federation, an average cost of one completed THI case ranges from $1,800 to $2,371, depending on the depth and severity of the lesion, while an average cost of a bed-day is $170 [3, 4].
Thus, the relevance of the THI problem in children and adolescents is beyond doubt from clinical and economic standpoints. At the same time, an actual assessment of the THI economic burden in the considered age category of patients depends on the outcomes of epidemiological studies, the results of which are influenced by a unified approach to their design and timing (duration). The development of a single design is difficult due to the lack of a unified classification of THI in children and youths.
In most classifications valid in Russia and abroad, THI is currently classified as a subsection of the of thermal injury in general, or (less often) as a thermal injury of the upper limb.
According to the International Statistical Classification of Diseases and Related Health Problems of the 10-th revision (ICD-10, 1995) [5], operating in Russia, and the new ICD of the 11-th revision adopted abroad (ICD-11, 2018) [6], THI is divided into three severity grades.
THI within epidermis constitutes grade I. Grade II encompasses THI spreading to the papillary layer of the dermis albeit preserved skin derivatives. Grade III involves THI with damage to all skin layers up to its own fascia, and in some cases, with damage to deep subfascial structures.
This classification was adopted by Russian NGO, Association of Combustiologists “The World without Burns”. However, some foreign associations of combustiologists (e.g., German Society for Burn Treatment, American Burn Association, European Burns Association) recommend using a modified classification: THI that involve solely the epidermis and do not require an assessment of the thermal damage area are classified as superficial (severity grade I); superficial partial THI, encompassing the epidermis and papillary dermis (severity grade II); deep THI, affecting the entire dermis and subcutaneous fat (severity grade III); THI affecting the underlying tissues, including muscles, fascia and bones (severity grade IV).
Unfortunately, a unified approach to the use of four grades of THI severity in clinical practice was hot developed yet, which makes it difficult to evaluate the results of ongoing epidemiological studies, in which THI often cannot be classified not only in terms of its severity, but also are not distinguished from thermal injuries of the upper limb. Although the approaches to surgical treatment in the acute and late periods of THI differ, compared with those for thermal injuries of other parts of the upper limb, we attempted to systematize the epidemiological studies of THI in children and adolescents, taking into account the above-mentioned classification problems and differences in the design of epidemiological studies employed by the scientific groups in Russia and abroad.
Due to high incidence of THI in children and youths, this issue is of a definite scientific and clinical interest. However, frequencies of THI occurrence in the pediatric population varies across the countries and regions, which prompted us to conduct this study.
The goal of our thematic overview was to systematize and update knowledge about the incidence of THI in children and youths in Russia and abroad.
Material and Methods
We analyzed domestic and foreign epidemiological studies published in the following databases: eLibrary, Google Scholar, PubMed, Springer, Scopus, Elsevier, Oxford Press, Clinical Case, Cochrane.
The thematic overview involved full-text articles in Russian and English, including original articles, thematic and systematic reviews, as well as Cochrane reviews.
The search for publications was carried out using the keywords and their combinations in Russian and English: burn, trauma, hand, arm, hand injury, thermal hand injury, frequency, incidence, prevalence, epidemiology.
The studies included the following age categories: children (male: 0-16 years old; female: 0-15 years old); adolescents (male: 17-21 years old; female: 16-20 years old). Despite our comprehensive search, it is possible that we overlooked some recent publications, or else they may have been unavailable to us.
We analyzed a total of 368 publications, which included 29 publications that corresponded to the goal of our research, in which the results of epidemiological studies of THI in children and adolescents were presented (Table 1).
Table 1. Results of epidemiological studies on thermal hand injury in children and adolescents of the Russian Federation and worldwide
|
Country/Region |
Sample size |
Frequency of occurrence, % |
Mean age (min; max), years old |
Reference |
||
|
Russian Federation |
|
|||||
|
Republic of Mordovia |
1,289 |
69.1 |
2.8 (1; 16) |
[2] |
|
|
|
Tyumen |
1,950 |
8.4 |
4.1 (< 1; 17) |
[9] |
|
|
|
Krasnodar |
272 |
29.7 |
(1; 18) |
[11] |
|
|
|
Tyumen |
3,059 |
11.1 |
4.0 (0.08; 17) |
[10] |
|
|
|
Voronezh |
30 |
40.0 |
(0.16; 1) |
[12] |
|
|
|
North America and South America |
|
|||||
|
USA |
70,302 |
0.11 |
(3.3; 0.7) |
[13] |
|
|
|
USA |
2,548,971 |
37.1 |
5.3 (0.7; 18) |
[14] |
|
|
|
USA |
255 |
36.0 |
1.9 (1; 5) |
[15] |
|
|
|
USA |
28,363 |
38.6 |
3.5 (1; 17) |
[16] |
|
|
|
USA |
3,193 |
29.5 |
11.8 (-; 18) |
[17] |
|
|
|
Canada |
1,039 |
56.0 |
4.25 (1; 5) |
[18] |
|
|
|
Canada |
1,183 |
58.9 |
8.15 (1; 19) |
[19] |
|
|
|
Europe |
|
|||||
|
UK |
407 |
– |
(0; 15) |
[26] |
|
|
|
Greece |
25 |
96.0 |
3.6 (0.91; 14) |
[25] |
|
|
|
Spain |
287 |
51.2 |
3.8 (0.08; 17) |
[20] |
|
|
|
Belarus |
40 |
27.5 |
3.8 (0.41; 17) |
[22] |
|
|
|
Belarus |
40 |
22.5 |
(1; 17) |
[21] |
|
|
|
Turkey |
419 |
49.9 |
4.02 (4; 17) |
[24] |
|
|
|
Turkey |
758 |
10.0 |
6.4 (0.08; 18) |
[23] |
|
|
|
Western Pacific countries |
|
|||||
|
China |
470 |
29.5 |
(1; 10) |
[27] |
|
|
|
China |
111 |
61.5 |
2.08 (0; 18) |
[28] |
|
|
|
Australia |
25,098 |
21.1 |
3 (1; 16) |
[30] |
|
|
|
Korea |
11,667 |
43.7 |
5.5 (0.08; 6) |
[29] |
|
|
|
Southeast Asia |
|
|||||
|
Taiwan |
3,425 |
10.0 |
4.02 (1; 5) |
[32] |
|
|
|
Pakistan |
85 (76/9) |
92.9 |
10.47 (1; 15) |
[33] |
|
|
|
India |
77 |
59.7 |
11.52 (3; 16) |
[31] |
|
|
|
Mediterranean |
|
|||||
|
Saudi Arabia |
33 |
100 |
9 (6; 12) |
[34] |
|
|
|
Lebanon |
179 |
12.3 |
5.5 (0.08: 19) |
[35] |
|
|
|
Africa |
|
|||||
|
South Africa |
994 |
33 |
3.4 (0; 13) |
[36] |
|
|
In addition, this thematic overview included earlier publications of historical interest, as well as some original studies in children and adolescents with thermal injury highlighting issues of clinical interest (frequency of THI localization on the dorsal and palmar surfaces of the hand, frequency of THI depending on the damaging factor, etc.), but with a small sample size. Such publications were analyzed by us in the Discussion section.
We used the classification of the World Health Organization (WHO) [7] and the classification of the Russian Federation regions [8]. According to them the regions of the world and of the Russian Federation, where epidemiological studies of THI in children and adolescents have been carried out, were identified (Figures 1 and 2).
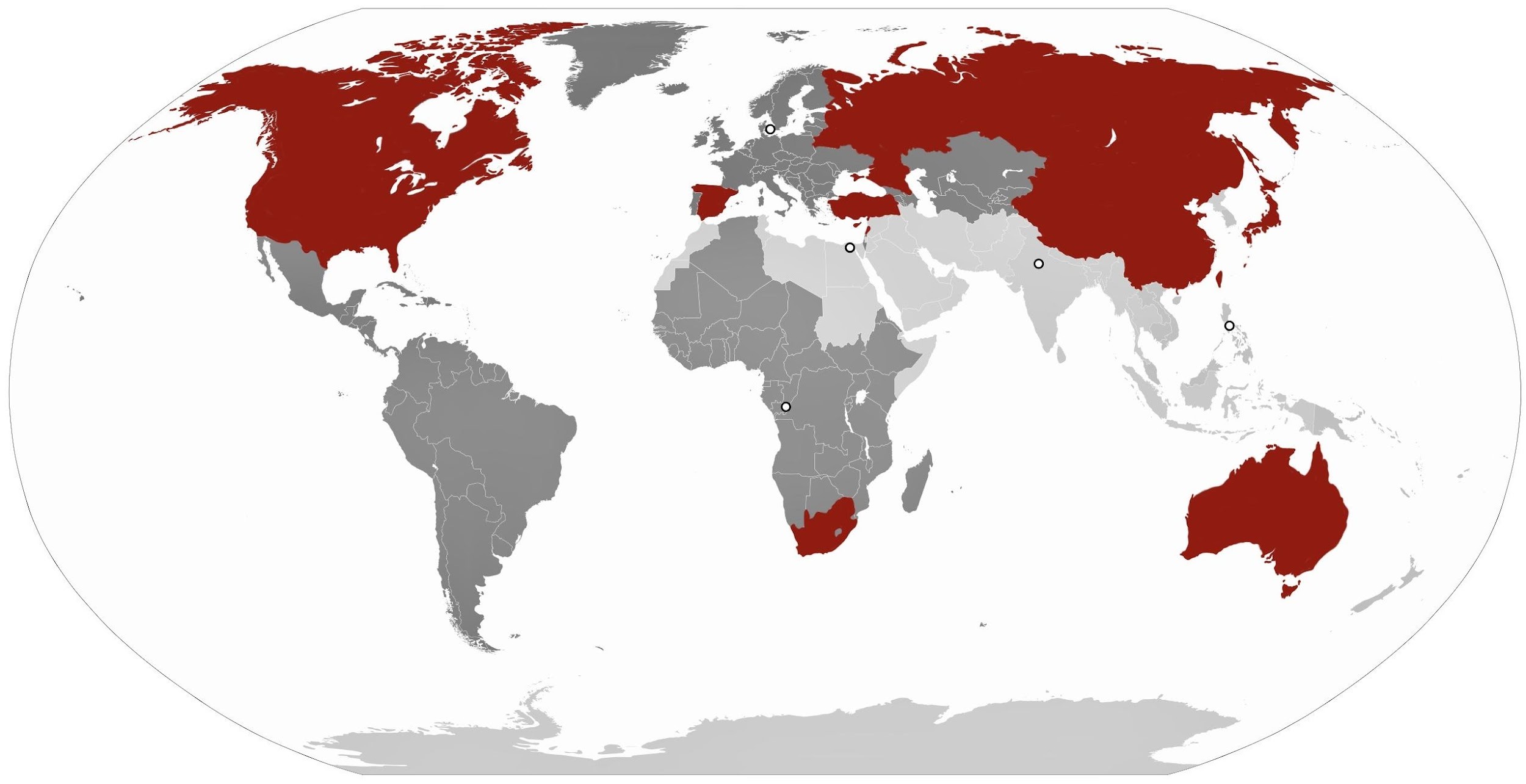
Figure 1. Regions of the world where epidemiological studies of thermal hand injury in children and youths have been conducted.

Figure 2. Regions of the Russian Federation where epidemiological studies of thermal hand injury in children and youths have been conducted.
Results
Russian Federation
We found and analyzed 5 epidemiological studies performed in the Russian Federation (one in the Republic of Mordovia [2]; two in Tyumen [9, 10]; one in Krasnodar [11]; and one in Voronezh [12]). Only three of them corresponded to the goals of our thematic overview: the Republic of Mordovia [2] and Tyumen [9; 10]. We also revealed and analyzed, but excluded from subsequent statistical processing, one more study, since it involved patients aged 1-65 years; however, this research is of clinical interest and will be considered further on in this review [11].
Also, one more epidemiological study was analyzed, but we did not include it in the statistical analysis due to a small sample size (n=30, only infants from 2 months to 1 year of age). However, this study was also of clinical interest; hence, it will be covered in the Discussion section [12].
A total of 6,783 cases of thermal injury were analyzed, 1,252 of which were cases of THI in children and adolescents. The age of the patients varied from 0.08 [10] to 17 years [10]. The mean age in children and adolescents with THI in Russia ranged from 2.8 in the Republic of Mordovia [2] to 4.1 in Tyumen [9] and constituted 3.6 years. The sample size ranged from 1,289 people [10] to 3,059 people [2], and the average sample size was 2,100. The incidence of THI among other cases of thermal injury ranged from 8.4% in Tyumen [9] to 69.1% [2] in the Republic of Mordovia. The average incidence of THI in children and youths living in the Russian Federation was 29.5%.
Countries of the Americas
For the countries of the Americas, we found 7 epidemiological studies, including: 5 in the USA [13-17] and 2 in Canada [18, 19].
We did not find any available results of studies performed in the countries of South America. Sample sizes varied from 255 [15] to 2,548 [14] people; age of children and adolescents ranged from 0.7 [13] to 19 years [19]; mean age was 5.45 years; and duration of studies varied from 1 year [16] to 24 years [14]. Overall, we analyzed 2 cases included in these epidemiological studies. Statistical processing was difficult due to the heterogeneity of the samples and to the fact that these studies included patients observed both at one [15] and at several medical centers [14]. A total of 955,893 children and adolescents with THI were identified, which accounted for 36.0% of cases from the entire sample. Besides, we discovered one epidemiological study of electrical burns of the upper limb [19], which did not correspond to the design of our research and thereby was excluded from further statistical analysis. However, the pathological changes and consequences of electrical burns of the hand are quite similar to those in THI; hence, this study will be covered in our further discussion.
European countries
The search brought up 7 epidemiological studies for European Countries: one in Spain [20]; two in the Republic of Belarus [21, 22]; and 2 in Turkey [23, 24]. We excluded two studies from further statistical analysis: one performed in Greece [25] with a small sample of 25 people and a short follow-up period of 6 months and another conducted in England [26] long ago (in 1984) and without specifying THI in children and adolescents. However, these two studies are of clinical and historical interest and will be reviewed in the Discussion section.
Overall, the analysis included 5 epidemiological studies involving 1,544 children and youths with thermal injury, including 481 cases of THI.
The sample size ranged from 40 people in Belarus [22] up to 758 people in Turkey [23]. The age of patients ranged from 1 month [23] to 18 years [23], and the mean age was 5.45 years.
The incidence of THI in children and youths in Europe was 29.3%.
Western Pacific countries
In the Pacific region, we found 4 epidemiological studies, including: 2 in China [27, 28], one in Korea [29], and one in Australia [30].
The age of patients ranged from 1 month [27] to 16 years [30]. The mean age was 4.04 years. The sample size varied from 111 people [28] to 25,098 people. [30]. The age of children and youths in one of the studies performed in China was limited to the age period from 1.25 years to 3.75 years, although the sample size (n=11) and duration of the study (1 year) were sufficient [28]. Such differences in the sample sizes of epidemiological studies in our analysis were due to the fact that the chosen period of data analysis was very variable: from one year [28] to ten years [30].
Overall, we analyzed 37,346 cases of thermal injury in children and adolescents, including 10,611 cases of THI. The incidence of THI in the pediatric population of the Pacific Rim ranged from 21.1% in Australia [30] to 61.5% in China [28], with an average incidence of 28.4%.
Southeast Asia
In the countries of Southeast Asia, we found and analyzed 3 epidemiological studies – one for each of three countries: India [31], Taiwan [32] and Pakistan [33]. Although two of these studies included patients with THI resulting from exposure to high temperatures caused by electrical trauma (exposure to electric current), we excluded them from the analysis. However, due to the fact that the mechanism of thermal damage to the hand and the consequences of THI could be comparable to those of THI caused by exposure to other thermal factors, we will consider these studies further on in the Discussion section.
Overall, we analyzed 3,425 cases of thermal injury in children and youths, all of which were cases of THI. The mean age was 4.02 years, the maximum age (5 years) was recorded in a study conducted by colleagues from Taiwan [32]. The minimum age for children was 1 year.
The incidence of THI in children and youths in Southeast Asia was 10.0% (Taiwan) [32]. Due to the fact that we found only one study that met the criteria for our thematic review in the region, extrapolation of epidemiological studies to the entire region is provisional.
Countries of Mediterranean region
For the countries of the Eastern Mediterranean, we found 2 epidemiological studies performed in Saudi Arabia [34] and Lebanon [35]. The study conducted in Saudi Arabia could not be fully classified as epidemiological, since the entire sample was represented only by children and adolescents with THI, but did not involve other thermal injuries. This prevented the researchers from commenting on the frequency of THI among other thermal injuries in their country. However, this study is of clinical interest and makes it possible to assess the incidence of burns of the dorsal and palmar surfaces of the hand, along with a total damage to the hand; hence, we will consider it in the Discussion section.
A total of 179 cases of thermal injury in children and youths living in Lebanon were involved in the statistical analysis, including 20 cases of THI. The age of the patients ranged from 1 month to 19 years, with a mean age of 5.5 years. The average frequency of THI was 12.3%. Because we analyzed just one epidemiological study in the Mediterranean region, extrapolation of the obtained results to the entire region is provisional.
Africa
For African countries, we found only one available epidemiological study in the Republic of South Africa (SAR), including children and adolescents with THI [36]. This study was conducted in only one city (Cape Town) and included 994 children and youths aged from 0 to 13 years, with 328 cases with THI. The mean age of children and youths was 3.4 years. The incidence of THI in children and adolescents in Africa (according to the data for South Africa) was 33.0%.
Due to the fact that we found solely one study for the African region, extrapolation of epidemiological studies to the entire region is provisional.
Discussion
A total of 21 epidemiological studies were analyzed, performed in the Russian Federation (3) and abroad (18). Although, sensu the classification of WHO regions, the Russian Federation belongs to the European Region, in this thematic review, however, epidemiological studies in our country were singled out into a separate category for subsequent analysis and comparison with the results obtained in other regions of the world.
The average incidence of THI was 25.5% in children and youths worldwide. At the same time, the average frequency of THI in children and adolescents living in the Russian Federation was 18.5% (Figure 3), which was comparable to European countries (29.3%) and Western Pacific countries (28.4%). However, in other countries of the world, epidemiological rates were statistically significantly higher (from 33.0% in the countries of Africa to 36.0% in America). Due to the fact that sensu WHO classification Russian Federation belongs to the European region, we have made an amendment to epidemiological studies in European countries, taking into account the results of Russian studies. Accordingly, the average incidence of THI in children and youths in the European region declined to 29.4%.

Figure 3. Frequency of thermal hand injury occurrence in children and youths of the Russian Federation.
Thus, the obtained values of THI in children and adolescents worldwide were distributed along the following gradient: countries of Southeast Asia (10.0%); Mediterranean countries (12.3%), European countries (23.9%), Western Pacific countries (28.4%), Africa (33.0%), and the Americas (36.0%) (Figure 4).
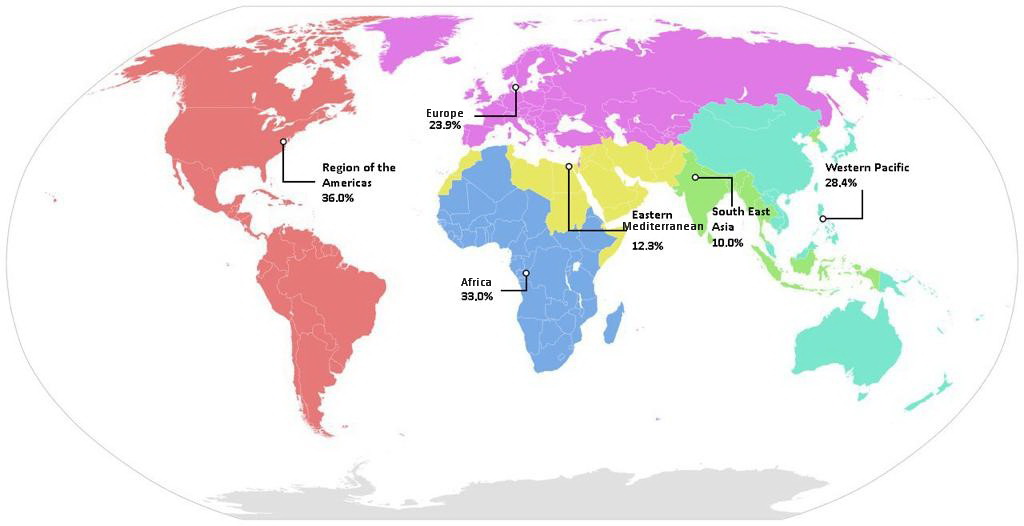
Figure 4. Frequency of thermal hand injury occurrence worldwide.

The limitations of our research are represented by the differences in design, sample size, age of enrolled patients, and duration of epidemiological studies conducted in different countries and regions worldwide. For instance, a study of the incidence of THI in children and adolescents in Greece was performed with the inclusion of 25 people and a short observation period of 6 months [25]; whereas a larger study in England [26] included children and youths along with the adults, but without isolating children and adolescents into a separate group when analyzing the incidence of THI. Therefore, we excluded such epidemiological studies from subsequent statistical processing, even though they were of clinical interest. It is likely that these limitations could explain the wide variation in the average incidence of THI. However, it should be taken into account that the frequency of THI in children and adolescents may be influenced by ethnic, cultural and other differences (including the differences in the nature of the upbringing and care of children and teenagers), and the type of thermal impact (liquid, flame, contact with hot objects, etc.). We did not find large multicenter studies of THI in children and adolescents with a single design for the analyzed period of time.
The mean age of children included in epidemiological studies ranged from 3.5 years in Africa and 3.6 years in Russia to 5.5 years in the Mediterranean countries. The mean age of children and adolescents with THI in Europe, including Russia, was 4.5 years. The mean age of children and youths with THI by region of the world was distributed as follows: Africa – 3.4 years, Southeast Asia – 4.02 years, Western Pacific countries – 4.04 years, Europe – 4.5 years, Americas – 5.45 years, Mediterranean countries – 5.5 years.
When analyzing epidemiological studies, we also paid attention to the localization of THI in children and adolescents. According to the results of the research conducted by R.G. Babichev et al. [11], the frequency of THI with localization on the dorsal surface of the hand was 29.7% of THI with other localization on the hand.
D.V. Chekmareva et al. [12] studied the incidence of THI in infants (from 2 months up to 1 year old) and showed that the incidence of THI in that population was 40%.
Analyzing the available studies regarding the prevalence of THI, we found several studies (one in Canada [19], one in India [31], and one in Pakistan [33]), reflecting the incidence of thermal damage to the hand as a result of exposure to electric current. Due to the fact that, according to the current classification of thermal injury [37], electrical injury is classified as a separate group, we analyzed these studies separately and included them in this thematic review only because their long-term consequences and impaired functioning of the hand were similar to the consequences of THI. A total of 1,345 cases of thermal injury due to exposure to electric current in children and youths, including 821 cases of THI, were analyzed. The incidence of THI in children and adolescents due to exposure to electric current was 61.0%. The mean age of children and adolescents was 7.8 years. The minimum and maximum ages in that population was 1 year [34] and 19 years, respectively [19]. Thus, the average frequency of THI due to electric current in children and adolescents in a comparable age group was almost two times higher than of THI due to other causes.
Conclusion
The issue of THI in the child population is relevant in all regions worldwide. However, scientific and clinical interest in conducting epidemiological studies varies among different countries and regions of the world, including the Russian Federation. The mean incidence of THI from among other thermal injuries in children and adolescents worldwide is quite high and makes up for about a one-third of cases (31.3%). This explains an importance of this interdisciplinary issue not only in combustiology, but also in traumatology and plastic surgery, because the long-term consequences of THI in people who experienced it in their childhood or adolescence largely depend on the close interaction of physicians of various specialties.
Conflict of Interest
No conflicts of interest are reported by the authors.
- Jeschke MG, van Baar ME, Choudhry MA, Chung KK, Gibran NS, Logsetty S. Burn injury. Nat Rev Dis Primers 2020; 6(1): 11. https://doi.org/10.1038/s41572-020-0145-5.
- Borisov IG, Karpushkina PI, Pigachev AV. Features of burns in children of the Republic of Mordovia. In: 46th Ogarev’s Readings: Proceedings of Scientific Conference. Part 2. Saransk. 2018: 276-280. Russian. https://www.elibrary.ru/item.asp?id=35281555.
- Karimi H, Motevalian SA, Momeni M, Ghadarjani M. Financial burden of burn injuries in Iran: A report from the burn registry program. Ann Burns Fire Disasters 2015; 28(4): 310-314. https://pubmed.ncbi.nlm.nih.gov/27777552.
- Unizhayeva AYu, Martynchik SA. Medical economic evaluation of hospital costs linked to quality of inpatient care for burning injury. Social Aspects of Population Health 2012; (6(28)): 8. Russian. https://www.elibrary.ru/item.asp?id=18765825.
- International Classification of Diseases 10th Revision (ICD-10). Russian. https://mkb-10.com.
- International Classification of Diseases 11th Revision. The global standard for diagnostic health information. https://icd.who.int/en.
- World Health Organization. https://en.wikipedia.org/wiki/World_Health_Organization.
- Database of cities, regions and federal districts of the Russian Federation in MySQL. Russian. https://snipp.ru/handbk/geo-russia.
- Akselrov MA, Razin MP, Belan YuB, Akselrov AM, Svazyan VV, Muratova NG. Medical and social aspects of thermal injury in children. Medical Newsletter of Vyatka 2015; (4(48)): 32-35. Russian. https://www.elibrary.ru/item.asp?id=25586592.
- Sakharov SP. Thermal injury in children of the Tymen region: medico-social problems. Russian Journal of Pediatric Surgery, Anesthesia and Intensive Care 2012; 2(3): 68-71. Russian. https://www.elibrary.ru/item.asp?id=18634846.
- Babichev RG, Bogdanov SB, Savchenko YP. Topical issues of surgical treatment of burns dorsum of the hand. Kuban Scientific Medical Bulletin 2016; (2): 20-24. Russian. https://www.elibrary.ru/item.asp?id=26374312.
- Chekmareva DV, Vecherkin VA, Kuznetsova VO, Kovalenko ES. Features of burns in infants. In: Topical Issues of Medicine in Modern Conditions: Collection of scientific papers based on the results of the III international scientific and practical conference. Saint Petersburg, Russia: Innovative development center of education and science. 2017; 36-38. Russian. https://elibrary.ru/item.asp?id=28428290.
- Marchalik R, Rada EM, Albino FP, Sauerhammer TM, Boyajian MJ, Rogers GF, et al. Upper extremity friction burns in the pediatric patient: A 10-year review. Plast Reconstr Surg Glob Open 2018; 6(12): e2048. https://doi.org/10.1097/gox.0000000000002048.
- Mitchell M, Kistamgari S, Chounthirath T, McKenzie LB, Smith GA. Children younger than 18 years treated for nonfatal burns in US emergency departments. Clin Pediatr (Phila) 2020; 59(1): 34-44. https://doi.org/10.1177/0009922819884568.
- Zamboni WA, Cassidy M, Eriksson E. Hand burns in children under 5 years of age. Burns. 1987; 13(6): 476-483. https://doi.org/10.1016/0305-4179(87)90227-0.
- Johnson SA, Shi J, Groner JI, Thakkar RK, Fabia R, Besner GE, et al. Inter-facility transfer of pediatric burn patients from U.S. emergency departments. Burns 2016; 42(7): 1413-1422. https://doi.org/10.1016/j.burns.2016.06.024.
- Myers J, Lehna C. Effect of fireworks laws on pediatric fireworks-related burn injuries. J Burn Care Res 2017; 38(1): e79-e82. https://doi.org/10.1097/bcr.0000000000000435.
- Garland K., Nahiddi N, Trull B, Malic C. Epidemiological evaluation paediatric burn injuries via an outpatient database in Eastern Ontario. Burns Open 2018; 2(4): 204-207. https://doi.org/10.1016/j.burnso.2018.06.004.
- Böhre М, Stewart SA, Hurley KF. Epidemiology of electrical and lightning-related injuries among Canadian children and youth, 1997-2010: A Canadian Hospitals Injury Reporting and Prevention Program (CHIRPP) study. CJEM 2018; 20(4): 586-591. https://doi.org/10.1017/cem.2017.49.
- Gómez GM, Carreño AP. Quemaduras de la mano en niños: experiencia de 5 años en una unidad de quemados pediátrica en bogotá - (hand burns in children: a 5 year experience in a pediatric burn unit in bogotá). Revista Colombiana de Cirugía Plástica y Reconstructiva 2021, 27(1). https://www.ciplastica.com/ojs/index.php/rccp/article/view/164.
- Krot AA, Shestel IV. Autograft as a method of surgical treatment of grade II-III a-b burns in children. In: Sikorsky AV, Khryshchanovich VYa, Eds. Actual problems of modern medicine and pharmacy 2019: Collection of materials LXXIII Intern. scientific-practical conference of students and young scientists. Minsk, Belarus: BSMU. 2019: 409. Russian. http://rep.bsmu.by/bitstream/handle/BSMU/28240/page_409.pdf.
- Kizukevich DL. Results of surgical treatment of children with thermal burns of the external body surfaces. In: Materials of the conference of students and young scientists dedicated to the memory of Professor Yu. G. Boyko. Grodno, Belarus: Grodno State Medical University. 2015: 258-259. Russian. http://elib.grsmu.by/handle/files/13401.
- Öztorun CA, Demir S, Azılı MN, Şenaylı A, Livanelioğlu Z, Şenel E. The outcomes of becoming a pediatric burn center in Turkey. Ulus Travma Acil Cerrahi Derg 2016; 22(1): 34-39. https://doi.org/10.5505/tjtes.2015.46417.
- Asena M, Akelma H, Salık F, Karahan ZA. The seasonal and monthly distribution of body limbs affected by burns in paediatric patients in southeast Turkey. Int Wound J 2019; 16(6): 1273-1280. https://doi.org/10.1111/iwj.13178.
- Tsiampouris I, Charcharidou M, Dousis E, Oikonomidi N, Makrygianni P, Vasilopoulos G, et al. Investigating the six-month incidence rate of burn disease in children in Greece. Cureus 2020; 12(10): e11192. https://doi.org/10.7759/cureus.11192.
- Green AR, Fairclough J, Sykes PJ. Epidemiology of burns in childhood. Burns Incl Therm Inj 1984; 10(5): 368-371. https://doi.org/10.1016/s0305-4179(84)80011-x.
- Liu M, Zhu H, Yan R, Yang J, Zhan R, Yu X, et al. Epidemiology and outcome analysis of 470 patients with hand burns: A five-year retrospective study in a major burn center in Southwest Chinа. Med Sci Monit 2020; 26: e918881. https://doi.org/10.12659/msm.918881.
- Li X, Wang X, Wang T, Yu H, Zhou Y, Wang H, et al. Multimethod assessing the prognosis affecting factors of hospitalized children with burns in Zunyi, southwest China. Wien Klin Wochenschr 2021; 133(5-6): 194-201. https://doi.org/10.1007/s00508-020-01676-z.
- Park JM, Park YS, Park I, Kim MJ, Kim KH, Park J, et al. Characteristics of burn injuries among children aged under six years in South Korea: Data from the Emergency Department-Based Injury In-Depth Surveillance, 2011-2016. PloS One 2018; 13(6): e0198195. https://doi.org/10.1371/journal.pone.0198195.
- Seah R, Holland AJ, Curtis K, Mitchell R. Hospitalised burns in children up to 16 years old: A 10-year population-based study in Australia. J Paediatr Child Health 2018; 55(9): 1084-1090. https://doi.org/10.1111/jpc.14347.
- Srivastava S, Patil AN, Bedi M, Tawar RS. Paediatric electrical burn injuries: Experience from a tertiary care burns unit in North India. Ann Burns Fire Disasters 2017; 30(3): 185-188. https://pubmed.ncbi.nlm.nih.gov/29849520.
- Chien WC, Pai L, Lin CC, Chen HC. Epidemiology of hospitalized burns patients in Taiwan. Burns 2003; 29(6): 582-588. https://doi.org/10.1016/s0305-4179(03)00133-5.
- Saaiq M. Epidemiology and outcome of childhood electrical burn injuries at Pakistan Institute of Medical Sciences Islamabad, Pakistan. J Burn Care Res 2016; 37(2): e174-e180. https://doi.org/10.1097/bcr.0000000000000202.
- Samhan AF, Abdelhalim NM, Elnaggar RK. Effects of interactive robot-enhanced hand rehabilitation in treatment of paediatric hand-burns: A randomized, controlled trial with 3-months follow-up. Burns 2020; 46(6): 1347-1355. https://doi.org/10.1016/j.burns.2020.01.015.
- Soni A, Pham TN, Ko JH. Acute management of hand burns. Hand Clin 2017; 33(2): 229-236. https://doi.org/10.1016/j.hcl.2016.12.001.
- Teo AI, Van As AB, Cooper J. A comparison of the epidemiology of paediatric burns in Scotland and South Africa. Burns 2012; 38(6): 802-806. https://doi.org/10.1016/j.burns.2012.04.010.
- Serror K, Chaouat M, Legrand MM, Depret F, Haddad J, Malca N, et al. Burns caused by electronic vaping devices (e-cigarettes): A new classification proposal based on mechanisms. Burns 2018; 44(3): 544-548. https://doi.org/10.1016/j.burns.2017.09.005.
Received 29 December 2021, Revised 28 February 2022, Accepted 24 March 2022
© 2021, Russian Open Medical Journal
Correspondence to Margarita A. Zhogina. E-mail: zhoginamargo@mail.ru.