Introduction
Dilated cardiomyopathy (DCM) is one of the leading causes of heart failure (HF). It is the most common type of cardiomyopathy characterized by cardiac enlargement: left ventricular end-diastolic dimension (LVEDD) >5.5 cm in men and >4.9 cm in women, end-systolic dimension (ESD) >3.5 cm, and reduced left ventricular ejection fraction (LVEF ≤40%) [1-3]. Numerous studies have shown that optimal medical therapy (OMT) is not sufficiently effective in patients with DCM [4]. Therefore, there is a need to develop alternative approaches and methods for treating chronic HF (CHF), such as cell therapy technology [5]. Mild chronic inflammation contributes to the pathogenetic progression of CHF, and increased levels of inflammatory biomarkers such as NT-proBNP and C-reactive protein (CRP) indicate the presence of CHF [6].
Stem cells (SCs) have anti-inflammatory and immunomodulatory effects. Two main types of stem cells have been described: embryonic stem cells and adult stem cells (ASCs) [7]. ASCs can be isolated from various tissues, such as umbilical cord, endometrial polyps, menstrual blood, bone marrow (BM), adipose tissue, etc. [8]. Mesenchymal stem cells (MSCs) are the most practical for experimental and potential clinical use, being attractive due to their ease of collection and the number of viable cells obtained [9]. MSCs have long-lasting anti-inflammatory and immunomodulatory effects [10].
Currently, there is limited information on the therapeutic efficacy of repeated MSC administration in HF, although the intravenous route of repeated MSC administration is the safest. A preclinical study comparing the efficacy of double and single MSC administrations in rats with DCM showed that double intravenous MSC administration resulted in better therapeutic efficacy and reduced inflammation in the rat hearts [11]. Our clinic performs autologous BM-derived MSC transplants to treat various diseases, including cardiovascular disease.
Scientific novelty: This is the first clinical trial to evaluate the effectiveness of repeated BM mesenchymal stem cell infusions for DCM.
Case description
Patient S, a 22-year-old man, was admitted to the clinic in August 2022 with complaints of dyspnea at rest (worsening in the horizontal position), swelling of both lower limbs, severe weakness, and palpitations.
Anamnesis morbi
Since the beginning of 2022, the aforementioned complaints first appeared after an acute respiratory viral infection. The patient denies the use of alcohol, illegal drugs, energy drinks, or cardiotoxic medications. There is no history of cardiovascular disease, diabetes mellitus, or cancer.
He received outpatient and inpatient treatment at his place of residence, along with receiving OMT for CHF: angiotensin receptor neprilysin inhibitors (ARNI), beta-blockers, mineralocorticoid receptor antagonists (MRAs), sodium-glucose transporter-2 inhibitors (SGLT2i), and loop diuretics). The patient was included in the main group of a randomized clinical trial of the scientific and technical program, Bone Marrow Mesenchymal Stem Cell Transplantation in Regenerative Medicine, approved by the Ethics Committee of the Astana National Scientific Medical Center and compliant with the 1964 Declaration of Helsinki, as amended (Figure 1).
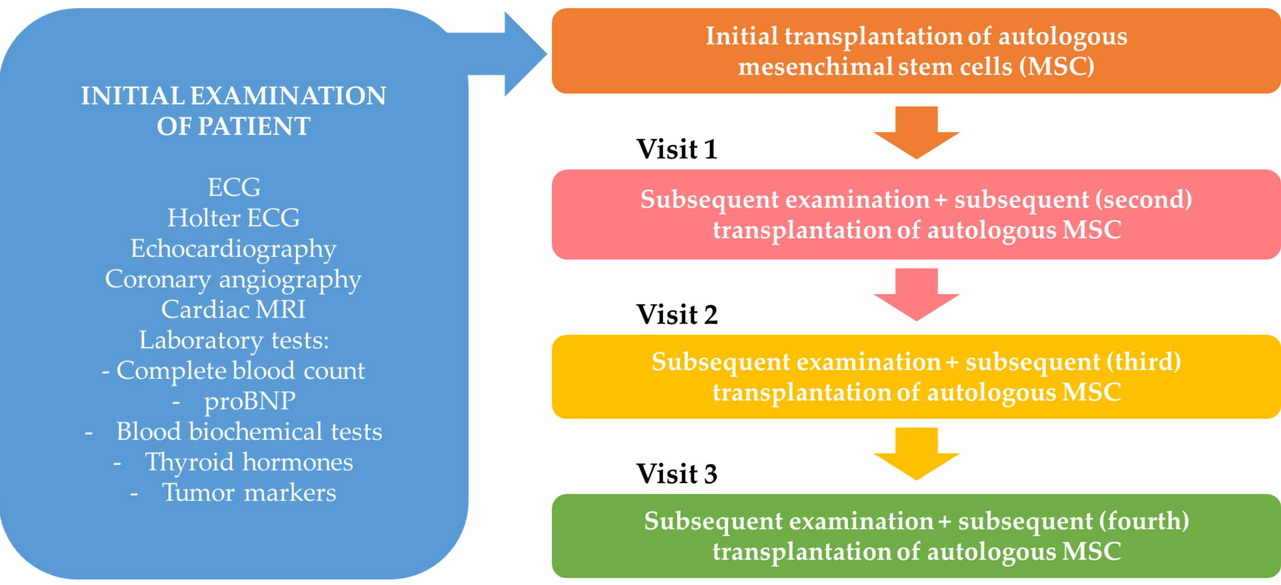
Figure 1. Study Design.
Upon admission to the clinic, the patient complained of general weakness, shortness of breath, and palpitations. His general condition was severe due to decompensated HF. Heart sounds were muffled, but the pulse was regular. Systolic heart murmur was present above the cardiac apex. Cardiac borders were as follows: right – 1.0 cm from the right edge of the sternum, left – 0.5 cm outside the midclavicular line, upper – at the level of the third rib. Pulse rate was 92 beats per minute (bpm); moderate tension and filling. Blood pressure: 120/70 mmHg.
Echocardiography revealed LVEF = 20%, heart chamber dilation (primarily of the left heart), diffuse hypokinesis, and a pericardial effusion of approximately 50 mL. Multispiral computed tomography (CT) of the coronary arteries revealed no signs of obstructive or stenotic vascular changes. NT-proBNP concentration was at the level of 25,000 pg/mL. Chest CT showed congestive changes in both lungs and bilateral hydrothorax. A six-minute walk test (6MWT) result of 105 meters corresponded to New York Heart Association (NYHA) Class IV. Based on the Minnesota Multiphasic Personality Inventory (MMPI) results, quality of life (QoL) was 82 points.
Laboratory and instrumental examination methods (August 2022)
Complete blood count (CBC): leukocytes – 8.35 10 μmol/L; erythrocytes – 6.18 10 μM/L; hemoglobin – 175.00 g/L; hematocrit – 51.90%; platelets – 263.00 10 μL/L; neutrophils – 63.30%; Lymphocytes – 29.80%; Eosinophils – 1.10%; immature granulocytes – 0.10%; erythrocyte sedimentation rate – 6 mm/h, C-reactive protein – 56 mg/L. Coagulogram, tumor markers and thyroid hormones were within normal limits. Tests for viral hepatitides B and C, and human immunodeficiency virus yielded negative results. Upon follow-up examination, NT-proBNP levels remain elevated – 12,567 pg/mL.
Electrocardiogram (ECG)
ECG revealed the sinus tachycardia with a heart rate of 91 bpm. Normal QRS axis.
Echocardiography
The left ventricle (LV) was dilated, but its walls were not thickened. Diffuse hypokinesia of the LV wall was observed. Global LV myocardial contractility was significantly reduced. LVEF = 20%. Tricuspid annular plane systolic excursion (TAPSE) = 13 mm. Maximum left atrial (LA) volume was 60 mL. Conclusion: LV dilation. Diffuse hypokinesia of the walls. Global LV myocardial contractility is significantly reduced by LVEF = 20%. Grade 1 mitral regurgitation.
Magnetic resonance imaging (MRI) of the heart with contrast
Conclusion: LV myocardium has a relatively uniform thickness with a uniform amplitude of wall motion in systole and diastole. With intravenous contrast administration in the delayed phase, no defects and abnormal areas of contrast-enhanced LV myocardium were detected (Figure 2). MRI indicated reduced global contractility of the LV myocardium (LVEF =17% by endocardial volume; LVEF =20% by blood volume). No abnormal structural changes in the LV myocardium were detected. Decreased stroke volume (52.4/53.4 mL), MCV (3.4/3.5 L/min), and cardiac index (2.1 L/[min×m2]) (Figures 3-4).
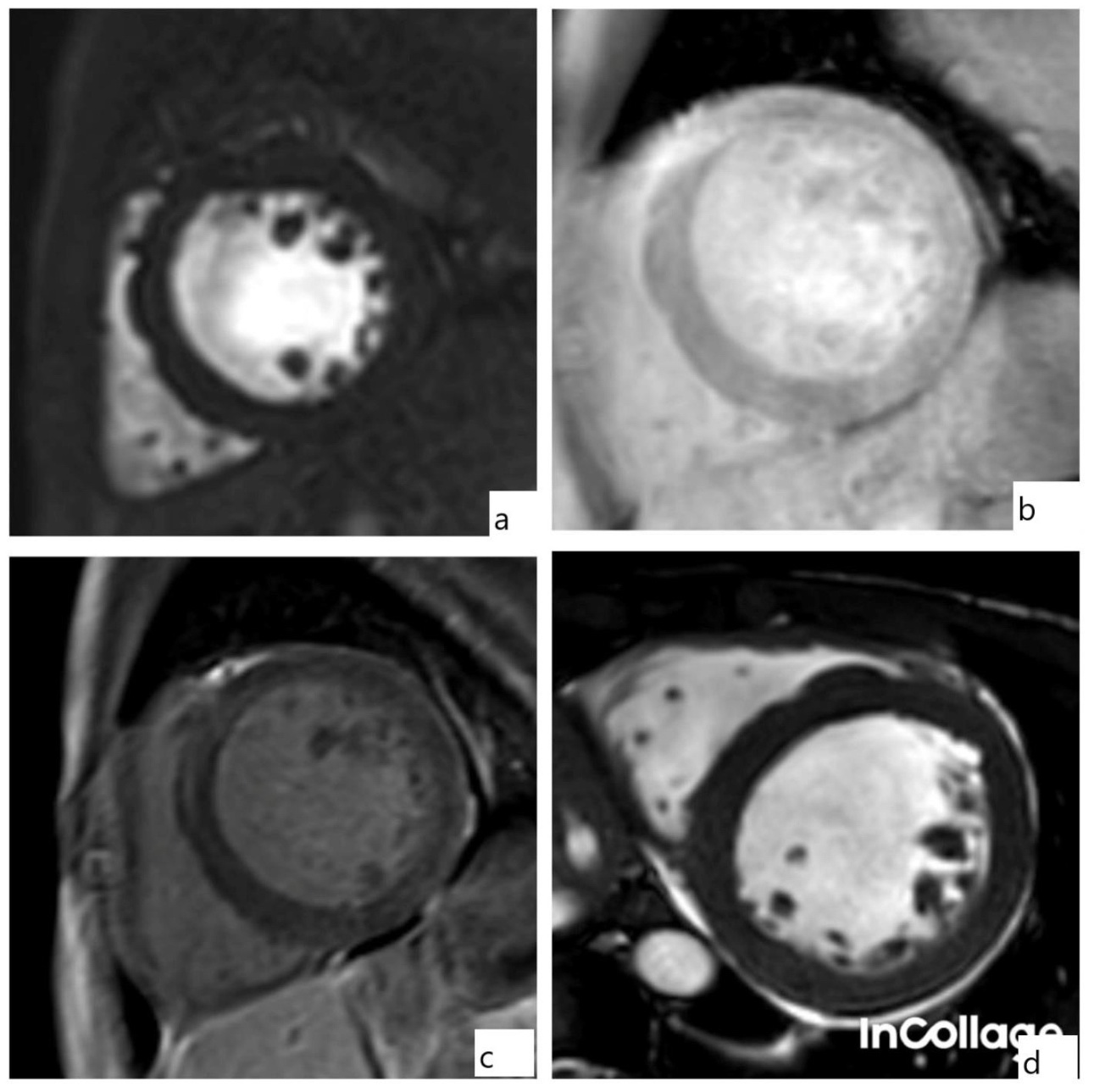
Figure 2. Cardiac magnetic resonance imaging (MRI), before cell therapy, a.) 23-year-old patient with dilated cardiomyopathy. Cardiac MRI, projection along the short axis of the left ventricle (LV) (Perfus). b.) projection along the short axis of the LV. c.) projection along the short axis of the LV. d.) projection along the short axis of the LV.
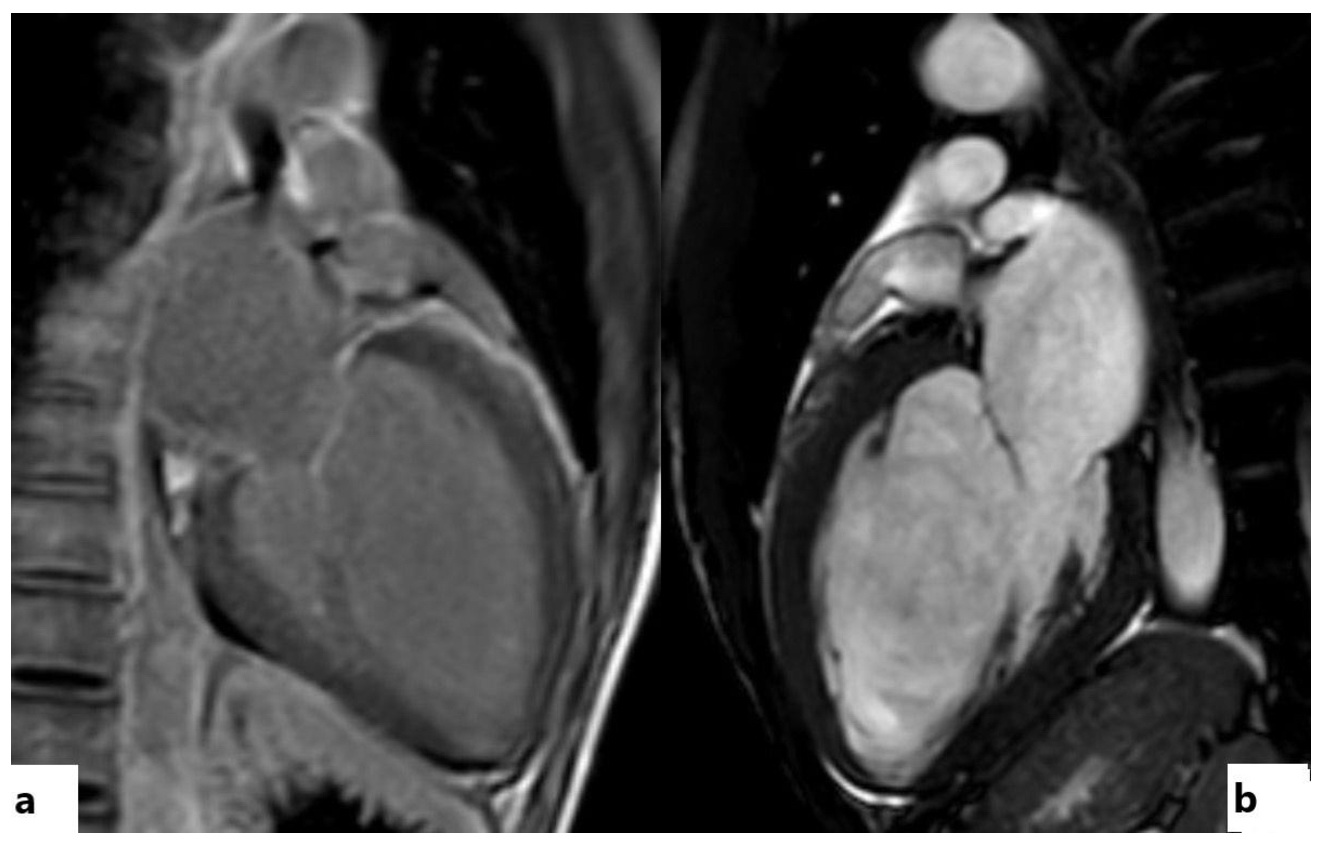
Figure 3. Cardiac magnetic resonance imaging (MRI), before cell therapy. 23-year-old patient with dilated cardiomyopathy, a.) Cardiac MRI, projection of the 4-chamber section of the left ventricle (LV). b.) projection of the 4-chamber section of the LV. c.) projection along the short axis of the LV. d.) projection along the short axis of the LV.
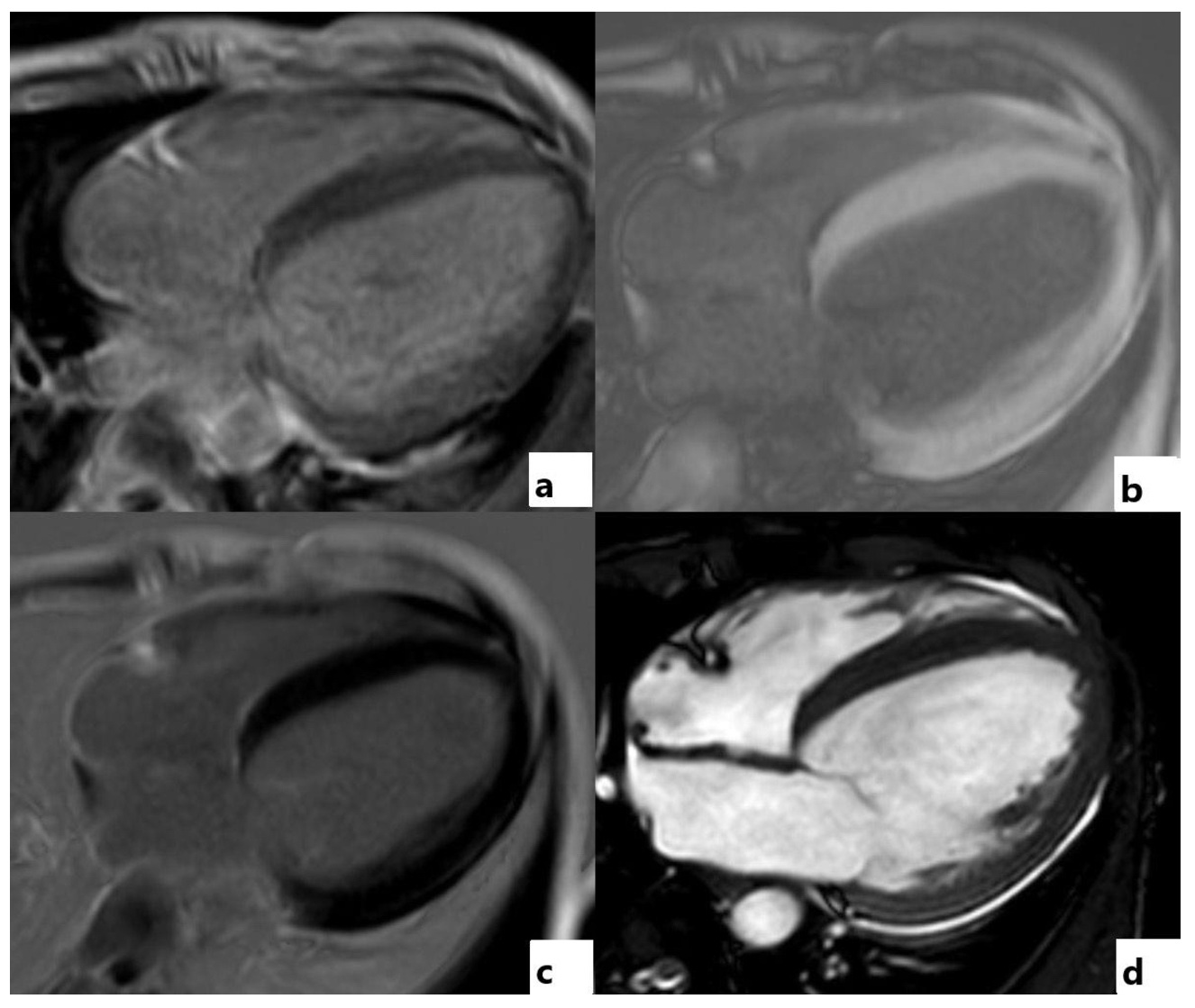
Figure 4. Cardiac magnetic resonance imaging (MRI), before cell therapy. 23-year-old patient with dilated cardiomyopathy, a.) Cardiac MRI, projection of the 4-chamber section of the left ventricle (LV). b.) projection of the 4-chamber section of the LV. c.) projection of the 4-chamber section of the LV. d.) projection of the 4-chamber section of the LV.
24-hour Holter monitoring
No arrhythmias were detected. Chest X-ray revealed no focal changes.
Surgical intervention (August 2022)
BM harvesting followed by autologous MSC transplantation was conducted as follows: harvesting was performed from the posterior third of the right iliac crest. 200 mL of BM was aspirated. The mononuclear stem cell fraction was isolated in the stem cell biotechnology laboratory. One day after BM harvesting, 110×106 mononuclear SCs were diluted in 200 mL of saline and administered intravenously to the patient.
Postoperatively, no typical specific complications were observed (such as cardiac arrhythmias, hematomas, bleeding, or allergic reactions). Subsequently, the patient was advised to continue OMT and repeat the MSC transplantation after four months. The patient underwent four courses of BM harvesting followed by autologous MSC transplantation at four-month intervals.
Observation
During the follow-up period, based on the data from four visits with four-month intervals (Table 1), the patient exhibited positive changes over a 2-year period. There were no complaints, and the patient’s general condition was satisfactory. There was no edema, and physical activity tolerance improved. HF severity decreased from Class IV to Class I (the patient could walk more than 505 meters during the 6MWT). His QoL improved according to the MMPI questionnaire (60 pts.).
Table 1. Patient visits for cell therapy at four-month intervals
|
Visit |
1st cell therapy (2022) |
2nd (4 months after the 1st cell therapy) |
3rd (8 months after the 1stl therapy) |
4th (12 months after the 1st cell therapy) |
|
|
Patient complaints |
Complaints of shortness of breath at rest, swelling of both lower limbs, severe general weakness, and tachycardia. |
Weakness; shortness of breath persists during exercise. |
There is an improvement in general condition; shortness of breath persists with moderate exertion. |
No complaints, no swelling. |
|
|
Heart rate, bpm |
92 |
90 |
70 |
79 |
|
|
BP, mmHg |
120/80 |
125/80 |
130/85 |
130/80 |
|
|
6MWT |
100 |
250 |
312 |
505 |
|
|
MMPI, pts. |
82 |
78 |
70 |
60 |
|
|
pro-BNP, pg/mL |
12567 |
6645 |
1506 |
125 |
|
|
Echocardiography |
EDV, mL |
210 |
209 |
168 |
135 |
|
ESV, mL |
161 |
163 |
117 |
58 |
|
|
EF, % |
20 |
22 |
30 |
53 |
|
|
Surgery |
Number of cells (in millions) |
110 |
100 |
99 |
98 |
|
Complications |
None |
None |
None |
None |
|
Heart sounds: muffled, without wheezing. Cardiac borders were within normal limits. Heart rate was 79 bpm. Blood pressure =130/80 mmHg. Control ECG: no changes. Laboratory tests revealed a significant decrease in NT-proBNP levels from 25,000 pg/mL to 125 pg/mL, and a normalization of C-reactive protein concentration from 56 mg/L to 4.8 mg/L.
Echocardiography (January 2025)
A significant decrease in heart chamber size was observed: EDD from 71 to 50 mm, ESD from 51 to 37 mm, EDV from 210 to 135 mL, ESV from 161 to 58 mL, LA from 37 to 32 mm. Contrariwise, we noted an increase in LVEF from 30 to 57%.
Follow-up MRI of the heart (2025)
Revealed a moderate LV systolic dysfunction, diffuse hypokinesia of all LV segments, and an increase in LVEF from 17-20% to 48-53%. Stroke volume, cardiac output, as well as cardiac and systolic indices were within normal limits. Myocardial mass decreased (hypertrophy regression) (Table 2) (Figure 5).
Table 2. MRI parameters before and after MSC transplantation
|
Parameter |
Before (2022) |
After (2025) |
Change |
||
|
EV |
BV |
EV |
BV |
||
|
LVEF % |
17 |
20 |
48 |
53 |
↑ |
|
Stroke volume, mL |
53.4 |
52.4 |
68.4 |
62.2 |
↑ |
|
Resting cardiac output, L/min |
3.5 |
3.4 |
5.4 |
4.9 |
↑ |
|
EDV, mL |
317.1 |
256.3 |
160.8 |
144.6 |
↓ |
|
ESV, mL |
264.0 |
203.9 |
111.6 |
81.9 |
↓ |
|
LV wall mass, g |
277.2 |
243 |
↓ |
||
|
Systolic index, mL/m² |
32.5 |
31.9 |
42.2 |
38.64 |
↑ |
|
Cardiac index, L/(min×m2) |
2.1 |
2.1 |
3.3 |
3.02 |
↑ |
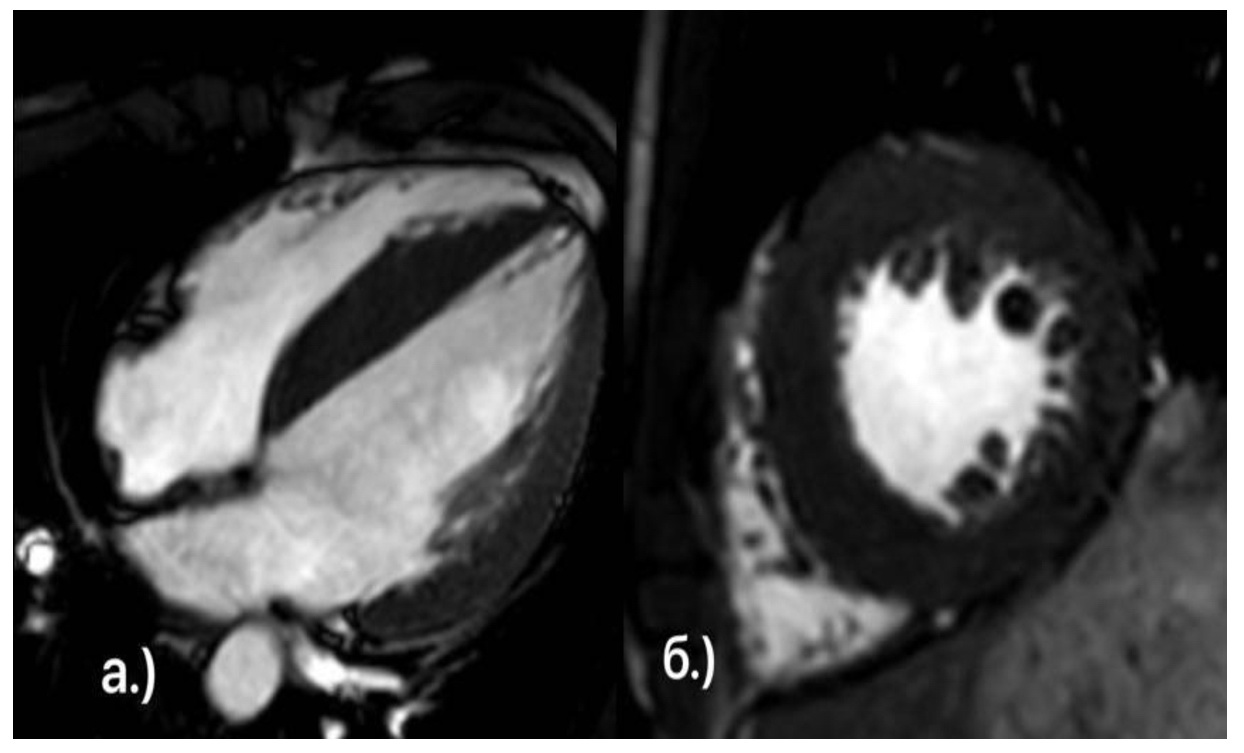
Figure 5. Cardiac magnetic resonance imaging (MRI), after cell therapy. 23-year-old patient with dilated cardiomyopathy, a.) Cardiac MRI, projection of the 4-chamber section of the left ventricle (LV). b.) short axis view of the LV.
Discussion
Cell therapy is not a routine treatment for DCM, but is used in cases where OMT is ineffective and where heart transplantation and left ventricular assist device placement are not possible. Repeated administration of autologous MSCs in combination with OMT in CHF leads to improvement in overall and local myocardial contractile function, as well as normalization of both left ventricular systolic and diastolic functions [11].
Cell therapy occupies an important place among developing regenerative technologies. Therefore, the treatment of CHF in DCM and CHF requires extensive specialized research. The results of many cell therapy studies are often presented as negative or modest. This is a common misconception that is detrimental to medical progress and must be dispelled.
Conclusion
Over a 2-year follow-up period, our patient demonstrated the effectiveness of repeat autologous mechanical blood vessel transplantation (4 visits) in the complex treatment of HF combined with OMT (ARNI, beta-blockers, MRAs, SGLT2i, and loop diuretics). This included improved physical activity tolerance, the absence of dyspnea (with moderate exertion) and edema, and the elimination of the need for diuretics. A decrease in NYHA HF Class from IV to I was observed.
Echocardiography data indicated an increase in LVEF from 20 to 53%, a decrease in HF marker (NT-proBNP) level in from 25,000 to 125 pg/mL, and an improvement in QoL, as measured by the MMPI questionnaire. A positive impact on the patient’s social life during the follow-up period, including starting a family and having a child, is also worth noting.
The presented case of DCM with CHF demonstrates the effectiveness of repeated infusions of autologous MSCs in a young patient. However, the question of the order and duration of cell therapy for cardiomyopathy and CHF dictates the need for specialized research. We hope that this clinical case will make at least a modest contribution to resolving this issue.
Ethical approval
All procedures performed in this study involving human participant were in accordance with the ethical standards of the institutional Ethics Committee and with the 1964 Declaration of Helsinki and its later amendments.
- Dellefave L, McNally EM. The genetics of dilated cardiomyopathy. Curr Opin Cardiol 2010; 25(3): 198-204. https://doi.org/10.1097/hco.0b013e328337ba52.
- Qin J, Zhang J, Lin L, Haji-Ghassemi O, Lin Z, Woycechowsky KJ, et al. Structures of PKA-phospholamban complexes reveal a mechanism of familial dilated cardiomyopathy. Elife 2022; 11: e75346. https://doi.org/10.7554/eLife.75346.
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016; 388(10053): 1545-1602. https://doi.org/10.1016/s0140-6736(16)31678-6.
- Vrtovec B, Poglajen G, Lezaic L, Sever M, Domanovic D, Cernelc P, et al. Effects of intracoronary CD34+ stem cell transplantation in nonischemic dilated cardiomyopathy patients: 5-year follow-up. Circ Res 2013; 112(1): 165-173. https://doi.org/10.1161/circresaha.112.276519.
- Nikiforova OL, Prikhodko LN, Kovalchuk PN. Clinical observation of a patient with chronic heart failure after mesenchymal stem cell implantation in outpatient conditions. Health and Ecology Issues 2021; 18(2): 131-139. Russian. https://doi.org/10.51523/2708-6011.2021-18-2-19.
- Adamo L, Rocha-Resende C, Prabhu SD, Mann DL. Reappraising the role of inflammation in heart failure. Nat Rev Cardiol 2020; 17(5): 269-285. https://doi.org/10.1038/s41569-019-0315-x. Erratum in: Nat Rev Cardiol 2021; 18(10): 735. https://doi.org/10.1038/s41569-021-00534-37.
- Baker DE, Harrison NJ, Maltby E, Smith K, Moore HD, Shaw PJ, et al. Adaptation to culture of human embryonic stem cells and oncogenesis in vivo. Nat Biotechnol 2007; 25(2): 207-215. https://doi.org/10.1038/nbt1285.
- Ding DC, Shyu WC, Lin SZ, Li H. Current concepts of adult stem cell therapy in stroke. Curr Med Chem 2006; 13(29): 3565-3574. https://doi.org/10.2174/092986706779026237.
- Ding DC, Shyu WC, Lin SZ. Mesenchymal stem cells. Cell Transplant 2011; 20(1): 5-14. https://doi.org/10.3727/096368910X.
- Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini F, Krause D, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006; 8(4): 315-317. https://doi.org/10.1080/14653240600855905.
- Gong C, Chang L, Sun X, Qi Y, Huang R, Chen K, et al. Infusion of two-dose mesenchymal stem cells is more effective than a single dose in a dilated cardiomyopathy rat model by upregulating indoleamine 2,3-dioxygenase expression. Stem Cell Res Ther 2022; 13(1): 409. https://doi.org/10.1186/s13287-022-03101-w.
- Dzholdasbekova A, Fedotovskikh G, Askarov M, Komsabakova B, Baigenzhina A, Kairatova A, et al. Systemic administration of autologous mononuclear precultured bone marrow cells in heart failure. J Clin Med Kaz 2015; 3(37): 14-18. Russian. https://www.clinmedkaz.org/article/systemic-administration-of-autologous-mononuclear-precultured-bone-marrow-stem-cells-in-heart-8777.
Received 21 February 2025, Revised 29 January 2026, Accepted 3 February 2026
© 2025, Russian Open Medical Journal
Correspondence to Meruert Latipbayeva. E-mail: meru_27_92@mail.ru.